REHAB · EP 01 · PAIN
Before You Listen
Episode Setup
- Topic in one line: the four-stage pain neuroanatomy, dorsal horn laminae and gate control theory, descending inhibition, central sensitization, and the core analgesic pharmacology (opioids, local anesthetics, nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, gabapentinoids, tricyclic antidepressants (TCAs), serotonin-norepinephrine reuptake inhibitors (SNRIs)) that every physiatrist needs cold on the American Board of Physical Medicine and Rehabilitation (ABPMR) Part I examination.
- Prerequisites: the Part 1 chapter (acute vs chronic pain, mechanism classification, and the pain lexicon), basic peripheral and central neuroanatomy, the spinothalamic tract, pre- and postsynaptic membrane physiology, voltage-gated calcium and sodium channels, and glucuronide versus oxidative drug metabolism.
- Runtime: Part 2 covers roughly the second half of the 1 hour 8 minute episode.
Vignette. A 58-year-old woman with a 5-year history of painful diabetic peripheral neuropathy returns to clinic. She describes constant burning in both feet at rest, intolerance of bedsheets brushing her toes, and a sharp shooting jolt that travels up her calf when she steps onto a cold tile floor. Her current regimen is acetaminophen 1 gram every 6 hours and oxycodone 10 mg three times daily; she still rates her pain 7 out of 10 and has gained 4 kg from inactivity. Glycated hemoglobin is 7.4 percent. Estimated glomerular filtration rate (eGFR) is 38 mL/min/1.73 m². On exam light touch on the dorsum of the foot is reported as painful, pinprick produces an exaggerated and prolonged response, and ankle reflexes are absent.
What is the mechanism-based pain category, which two terminology terms apply to her exam findings, what three first-line agents target the underlying mechanism, and which currently prescribed agent should be tapered first and why?
(Answer at the end of this chapter)
Section 2: The Four Stages of Pain Signaling, Nerve Fiber Types, and the Dorsal Horn
Bottom line: pain signaling proceeds through four sequential stages: transduction (nociceptor conversion of mechanical, thermal, or chemical stimuli into electrical signals; NSAIDs and local anesthetics act here), transmission (peripheral nerve to dorsal root ganglion to dorsal horn to spinothalamic tract to thalamus, with crossing within 1 to 2 levels), modulation (dorsal horn volume control with descending inhibition; TCAs and SNRIs amplify this stage), and perception (somatosensory cortex and limbic system); three nerve fiber types carry the signals: A-beta (12 to 14 micrometers, heavily myelinated, 30 to 60 m/s, touch and pressure, gate-closer), A-delta (6 to 8 micrometers, thinly myelinated, 10 to 15 m/s, sharp first pain), and C (less than 1 micrometer, unmyelinated, less than 1.5 m/s, dull burning second pain); the dorsal horn is organized in Rexed laminae I and II (substantia gelatinosa, C-fiber termination, opioid-receptor-rich, the rationale for intrathecal opioids) and III through V (A-beta and A-delta termination, wide dynamic range neurons that drive central sensitization).
The four stages of pain signaling are the scaffold for analgesic pharmacology; each stage is a drug target.
Transduction occurs at the peripheral nerve terminal where nociceptors convert noxious stimuli (mechanical, thermal, chemical) into action potentials. Tissue damage releases an “inflammatory soup” of prostaglandins, bradykinin, substance P, histamine, hydrogen ions, and potassium, which activate and sensitize nociceptors in peripheral sensitization. NSAIDs inhibit cyclooxygenase here; local anesthetics block voltage-gated sodium channels.
Transmission carries the signal along the peripheral nerve, through the dorsal root ganglion (DRG, the cell body of the primary afferent neuron and an emerging neuromodulation target), and into the dorsal horn. From the dorsal horn, second-order neurons cross within 1 to 2 spinal levels and ascend in the contralateral spinothalamic (anterolateral) tract to the thalamus, which is why a hemicord lesion produces contralateral loss of pain and temperature sensation a couple of levels below (Brown-Séquard pattern).
Modulation in the dorsal horn is the volume control center where ascending signals can be amplified or suppressed. Gate control theory operates here. Descending pathways inhibit transmission via 5-HT and NE release, the mechanism of TCAs and SNRIs.
Perception occurs in the brain. The somatosensory cortex generates the sensory-discriminative component (where it hurts); the limbic system (anterior cingulate cortex, insula) generates the affective-motivational component (suffering, behavioral response). Opioids, CBT, and mindfulness alter the subjective experience of pain at this stage.


Source: OpenStax College, Anatomy and Physiology, via Wikimedia Commons, CC BY 3.0
Nerve fiber types determine the clinical experience of pain: larger diameter conducts faster, myelination accelerates conduction, and small unmyelinated fibers carry the slowest signals.
A-beta fibers (12 to 14 micrometers, heavily myelinated, 30 to 60 m/s) carry touch, pressure, and vibration. They are not pain fibers, but A-beta activation closes the gate to C-fiber transmission (gate control theory). In central sensitization, A-beta input can be reinterpreted as painful, the mechanism of allodynia.
A-delta fibers (6 to 8 micrometers, thinly myelinated, 10 to 15 m/s) transmit sharp, well-localized, immediate “first pain”: what the patient feels the instant they step on a tack. They also respond to noxious thermal stimuli.
C fibers (less than 1 micrometer, unmyelinated, less than 1.5 m/s) transmit dull, burning, diffuse, poorly localized “second pain”: the deep ache that arrives after the initial sharp signal has passed. C fibers are polymodal (mechanical, thermal, chemical) and release substance P and calcitonin gene-related peptide (CGRP) at central terminals, contributing to neurogenic inflammation and central sensitization. The two-phase pain experience after acute injury directly reflects the conduction velocity difference between A-delta and C fibers.

Source: Helixitta, Wikimedia Commons, CC BY-SA 4.0
The dorsal horn is organized in Rexed laminae from superficial to deep. Laminae I and II form the substantia gelatinosa, the primary C-fiber termination zone, with lamina I housing nociceptive-specific neurons. The substantia gelatinosa is densely packed with mu-opioid receptors, which is why intrathecal and epidural opioids achieve profound analgesia at a fraction of the systemic dose; receptor density in laminae I-II is the entire rationale for neuraxial delivery.
Laminae III through V receive A-beta and A-delta input and contain wide dynamic range (WDR) neurons, which receive convergent input from both C and A-beta fibers and encode stimulus intensity rather than type. With repeated C-fiber input, WDR neurons become progressively more excitable and fire to normally non-painful stimuli, the cellular basis for allodynia and central sensitization.
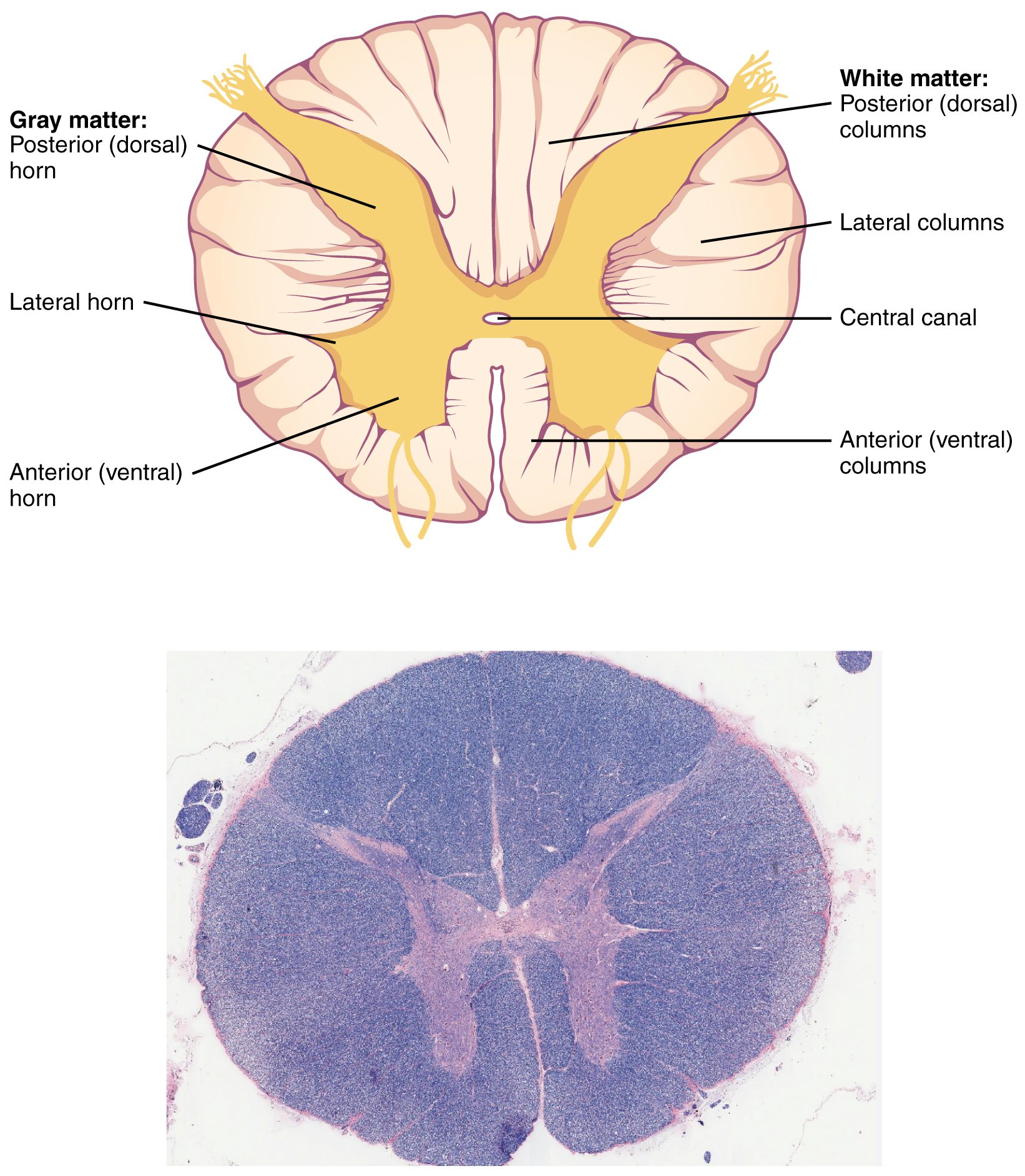
Source: OpenStax College, Anatomy and Physiology, via Wikimedia Commons, CC BY 4.0
Gate control theory (Melzack and Wall, 1965) remains the most influential framework in pain medicine. A-beta activation excites inhibitory interneurons in the substantia gelatinosa that “close the gate” to C-fiber pain traveling through the Lissauer tract. When A-beta activity falls, the gate opens and pain passes freely. Clinical applications: transcutaneous electrical nerve stimulation (TENS) preferentially activates A-beta fibers to close the gate; rubbing a sore area after bumping it works the same way; spinal cord stimulation (SCS) in the epidural space stimulates dorsal column A-beta fibers to close the gate centrally. The theoretical basis for TENS and SCS is always gate control theory.
High Yield — Stages, fibers, dorsal horn
- Four stages: transduction, transmission, modulation, perception. Each stage is a drug target.
- Fibers: A-beta (12-14 µm, myelinated, 30-60 m/s, touch and gate-closer); A-delta (6-8 µm, thin myelin, 10-15 m/s, sharp first pain); C (<1 µm, unmyelinated, <1.5 m/s, dull burning second pain).
- Substantia gelatinosa = laminae I-II = C-fiber termination plus opioid-receptor-rich = rationale for intrathecal opioids.
- WDR neurons in laminae III-V drive central sensitization and allodynia.
- Gate control theory (Melzack & Wall, 1965): A-beta closes the gate to C-fiber pain; basis for TENS and SCS.
- Spinothalamic crossing within 1-2 levels explains contralateral pain and temperature loss in cord lesions.