MEDREH · EP 11 · PASC
Before You Listen
Episode Setup
- Topic in one line: Post-Acute Sequelae of SARS-CoV-2 (PASC, also called Long COVID), defined as new, recurring, or persistent symptoms more than 12 weeks after the initial SARS-CoV-2 infection (4 weeks by some agencies); the multisystem symptom landscape (fatigue, brain fog, dyspnea, post-exertional malaise (PEM), postural orthostatic tachycardia syndrome (POTS), pain, anosmia/ageusia, mood and sleep disturbance, small fiber neuropathy); the single most important screening question — does activity precipitate a delayed (12-72 hour) symptom flare? — that diverges the rehabilitation algorithm into pacing-and-energy-conservation (with PEM, mirroring myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)) versus graded exercise therapy (without PEM, deconditioning pattern); POTS criteria (≥30 beats per minute (bpm) heart rate rise within 10 minutes of standing in adults, ≥40 bpm in adolescents, without orthostatic hypotension), nonpharmacologic management (2-3 liters fluid, 3-10 grams sodium, waist-high compression), and pharmacologic options (midodrine, fludrocortisone, beta-blockers, ivabradine); cognitive rehabilitation for brain fog using restorative and compensatory strategies; and the multidisciplinary clinic model led by physical medicine and rehabilitation (PM&R).
- Prerequisites: the deconditioning, deep vein thrombosis (DVT), and orthostatic intolerance material from REHAB-09; pulmonary rehabilitation principles from MEDREH-02; the ME/CFS literature on graded exercise therapy.
- Runtime: 1 hour 5 minutes.
Vignette. A 35-year-old woman, previously a healthy software engineer who ran 30 miles per week, presents to your post-COVID clinic 3 months after a mild outpatient SARS-CoV-2 infection that was managed at home with rest and acetaminophen. Since then she reports profound fatigue, “brain fog” with word-finding difficulty and lost trains of thought, and exercise intolerance. The pattern she describes is striking: on Tuesday she attempts to walk an extra block to the grocery store; on Wednesday and Thursday she is bedbound with crushing fatigue, headache, and lightheadedness. She has tried “pushing through” twice and each attempt produced a 4-day relapse. On examination, her supine heart rate is 72 with blood pressure 118/74. After 5 minutes of quiet standing, her heart rate rises to 118 with blood pressure 116/76, and she feels lightheaded with neck and shoulder discomfort. Her pulmonary examination, chest radiograph, and resting electrocardiogram (ECG) are unremarkable.
What single screening question separates her from a deconditioned patient and dictates the rehabilitation algorithm; what specific autonomic syndrome is illustrated by her standing test and what are its diagnostic criteria; what nonpharmacologic and pharmacologic management options apply; and why is graded exercise therapy contraindicated as a starting point?
(Answer at the end of this chapter)
Section 1: Defining PASC, Pathophysiology, and the Multisystem Symptom Landscape
Bottom line: PASC (Post-Acute Sequelae of SARS-CoV-2 or Long COVID) is a multisystem syndrome of symptoms persisting more than 12 weeks after acute infection (4 weeks per CDC); ~10-30 percent of infected individuals develop PASC (30-50 percent post-hospitalization, up to 70 percent post-ICU); risk factors are female sex, older age, obesity, diabetes, autoimmune disease, and number of acute symptoms; SARS-CoV-2 enters cells via the ACE2 receptor; the most common symptoms are fatigue (50-70 percent), brain fog (20-30 percent), dyspnea (25-40 percent), POTS, pain, sleep disturbance (40-50 percent), and mood disorders.
Post-Acute Sequelae of SARS-CoV-2 (PASC), commonly called Long COVID, is a multisystem syndrome whose temporal definition varies by guideline body — and the boards may use either threshold, so listeners should know both:
- CDC (US): symptoms persisting more than 4 weeks after acute SARS-CoV-2 infection.
- WHO post-COVID-19 condition criterion (2021 Delphi): symptoms persisting 3 months (~12 weeks) from initial infection with at least 2 months of symptoms not explained by an alternative diagnosis.
- NICE NG188 (UK) uses a three-tier framework: acute COVID-19 (≤4 weeks), ongoing symptomatic COVID-19 (4-12 weeks), and post-COVID-19 syndrome (>12 weeks).
The two thresholds are not contradictory — CDC and NICE flag the early subacute window earlier (after 4 weeks) for clinical attention, while WHO codifies the post-12-week threshold for formal post-COVID-19 condition diagnosis. The National Institutes of Health (NIH) RECOVER Initiative has standardized research criteria that bridge both frameworks. Regardless of the temporal cutoff, the core concept is consistent: a multisystem syndrome that persists well beyond expected acute viral recovery.
Epidemiology. Approximately 10-30 percent of all infected individuals develop PASC. Rates rise to 30-50 percent after hospitalization and up to 70 percent after ICU admission. PASC is not confined to severe acute illness; it occurs with meaningful frequency after mild and moderate infections, and acute illness severity does not reliably predict long-term sequelae. Risk factors include female sex, older age, pre-existing comorbidities (especially obesity, diabetes, autoimmune disease), and the number of acute symptoms during initial infection.
Pathophysiology. SARS-CoV-2 enters human cells via the angiotensin-converting enzyme 2 (ACE2) receptor, with the viral spike protein serving as the binding agent. The pathophysiology of PASC is incompletely understood but likely involves multiple overlapping mechanisms: persistent viral reservoirs in tissue, immune dysregulation and chronic inflammation (elevated interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-alpha), and interferon-gamma), autoimmunity triggered by molecular mimicry, endothelial dysfunction with microvascular thrombosis, and autonomic nervous system disruption. The mechanistic heterogeneity likely explains the wide variability in clinical presentation.
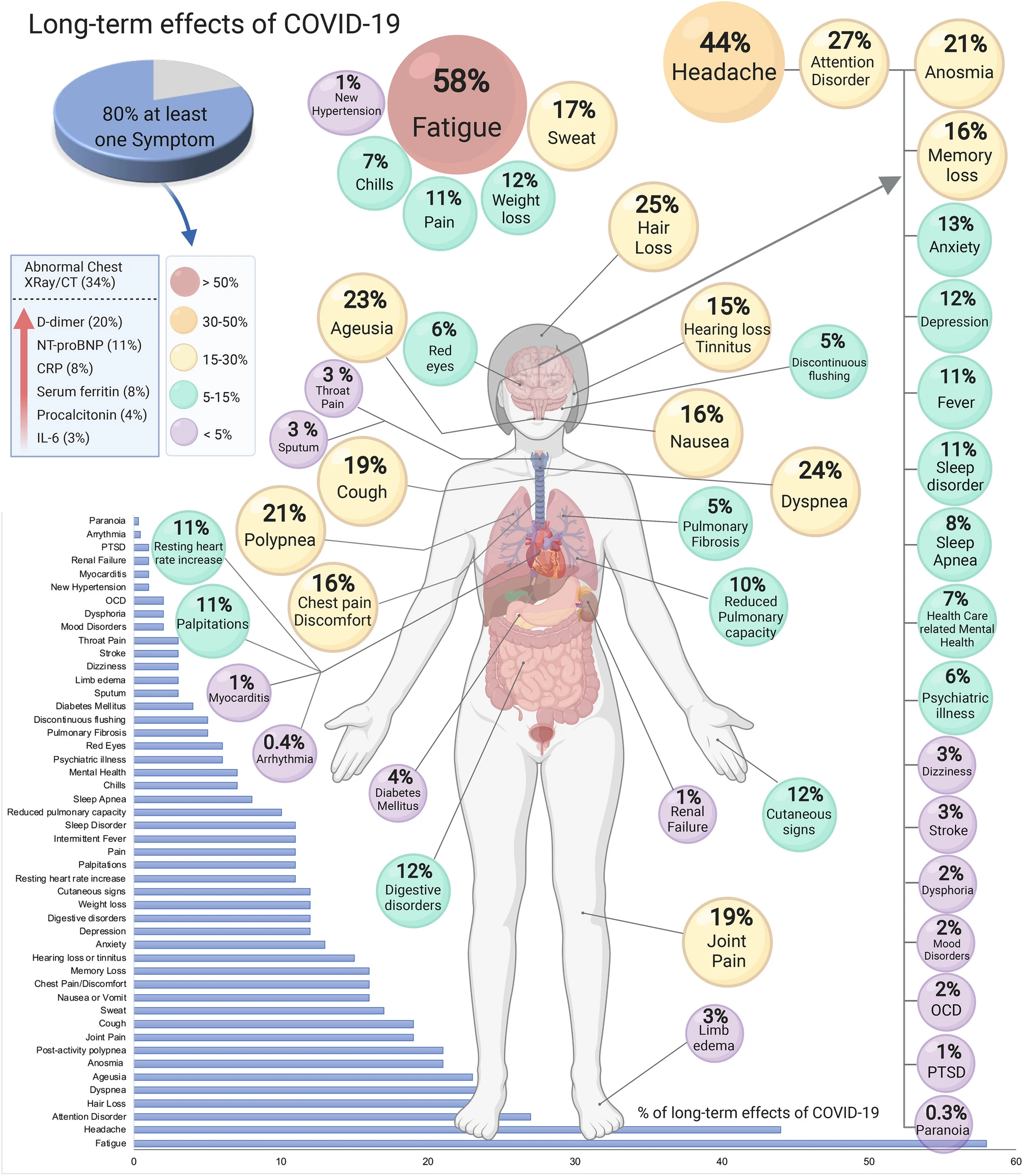
Source: Mikael Häggström, based on Lopez-Leon et al. 2021 (Nature Scientific Reports), Wikimedia Commons, CC BY 4.0

The symptom landscape spans more than 200 reported symptoms organized by organ system.
- Fatigue is the most common symptom, reported in 50-70 percent of affected patients. The fatigue of PASC is a profound, debilitating exhaustion disproportionate to activity, unrelieved by rest, and qualitatively different from any pre-infection fatigue. It shares clinical features with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and a significant subset of PASC patients meet formal ME/CFS criteria.
- Cognitive dysfunction (brain fog) affects 20-30 percent and is among the most functionally limiting symptoms. Affected domains include sustained attention, working memory, processing speed, executive function, and word-finding. Formal neuropsychological testing frequently reveals deficits even in patients describing only mild subjective complaints.
- Dyspnea and exercise intolerance occur in 25-40 percent. Pulmonary function tests and chest imaging may be entirely normal in a substantial proportion, suggesting dysfunctional breathing, deconditioning, and peripheral oxygen extraction impairment as major contributors. Cardiopulmonary exercise testing (CPET) is the most informative assessment, frequently revealing reduced peak oxygen consumption (VO2), chronotropic incompetence, and abnormal ventilatory responses.
- Autonomic dysfunction, particularly POTS, has emerged as a prominent feature.
- Pain syndromes (myalgia, arthralgia, headache, neuropathic pain) occur in 15-30 percent. Small fiber neuropathy has been confirmed by skin punch biopsy in subsets of patients with reduced intraepidermal nerve fiber density correlating with burning pain and autonomic symptoms.
- Psychiatric manifestations are highly prevalent: anxiety 30-40 percent, depression 20-30 percent, sleep disturbance 40-50 percent, PTSD 15-20 percent.
High Yield — Defining PASC

- PASC = multisystem syndrome with two accepted thresholds: >4 weeks (CDC) and >12 weeks (WHO post-COVID-19 condition; NICE post-COVID-19 syndrome). NICE uses a three-tier framework with ongoing symptomatic COVID-19 = 4-12 weeks. >200 reported symptoms.
- Prevalence: 10-30 percent of all infected; 30-50 percent after hospitalization; up to 70 percent after ICU. Severity of acute illness does NOT reliably predict PASC risk.
- Risk factors: female sex, older age, obesity, diabetes, autoimmune disease, more acute symptoms.
- Pathophysiology: SARS-CoV-2 enters via ACE2 receptor; mechanisms include persistent viral reservoirs, immune dysregulation, autoimmunity, endothelial dysfunction, autonomic disruption.
- Most common symptoms: fatigue (50-70%), brain fog (20-30%), dyspnea (25-40%), POTS, pain (15-30%), sleep disturbance (40-50%), anxiety (30-40%), depression (20-30%), PTSD (15-20%).
Mnemonic — “ACE2, the door SARS-CoV-2 walks through”

The spike protein of SARS-CoV-2 binds the angiotensin-converting enzyme 2 (ACE2) receptor on respiratory, vascular, cardiac, gut, and central nervous system endothelial cells. The same receptor distribution is what makes PASC multisystem rather than purely pulmonary; everywhere ACE2 is expressed is a potential source of late symptoms.