MSK · EP 24 · OSTEOPOROSIS
Before You Listen
Episode Setup
- Topic in one line: the pharmacologic and rehabilitative management of osteoporosis on the PM&R boards: bisphosphonate mechanism, oral administration discipline, atypical femur fractures and the drug holiday, denosumab and the rebound vertebral-fracture rule, teriparatide as the only purely anabolic agent, romosozumab’s dual mechanism with cardiovascular boxed warning, calcitonin’s narrow analgesic role in acute vertebral compression fracture, vertebral augmentation indications, and the fall-prevention bundle that cuts fractures more than any pill alone.
- Prerequisites: MSK-23 (WHO classification, Fracture Risk Assessment Tool (FRAX) thresholds, calcium and vitamin D targets, secondary causes), the bone remodeling unit (osteoblast, osteoclast, osteocyte), the receptor activator of nuclear factor kappa-B ligand (RANKL) pathway, the Wnt-signaling pathway and sclerostin, and the parathyroid hormone (PTH) effect of intermittent versus continuous exposure.
- Runtime: 47 minutes.
Vignette. A 72-year-old postmenopausal woman with severe osteoporosis (femoral neck T-score −3.2, two prior vertebral compression fractures) has been on subcutaneous denosumab 60 mg every 6 months for 4 years with stable bone mineral density (BMD). She develops a new dental abscess and her dentist requests that the denosumab be held for “at least a year” before extraction. She is on calcium 1200 mg/d, vitamin D 2000 international units/d, and a recent 25-hydroxy vitamin D is 38 ng/mL.
What is the major risk if denosumab is simply discontinued without a plan, what is the recommended sequencing strategy, what is the typical dental coordination plan in a patient on anti-resorptive therapy, what are the comparative roles of teriparatide, romosozumab, and bisphosphonates if a clinician decides she needs additional bone-building rather than only maintenance, and what counseling about an atypical femur fracture is appropriate?
(Answer at the end of this chapter)
Section 1: Bisphosphonates — Mechanism, Administration, Adverse Effects, and the Drug Holiday
Bottom line: bisphosphonates bind hydroxyapatite, are taken up by osteoclasts during resorption, and inhibit the mevalonate pathway to disrupt osteoclast cytoskeletal organization and induce apoptosis; oral alendronate, risedronate, and ibandronate plus intravenous (IV) zoledronic acid are the standard agents; oral dosing requires plain water on an empty stomach with the patient remaining upright for 30 minutes; the major adverse effects are esophagitis, atypical femur fractures (subtrochanteric/diaphyseal transverse fractures with prodromal thigh pain after ≥5 years of therapy), and rare osteonecrosis of the jaw (ONJ); a drug holiday is recommended after 5 years of oral therapy or 3 years of IV therapy.
Bisphosphonates are the first-line pharmacologic treatment for osteoporosis. They are synthetic analogs of pyrophosphate that bind avidly to hydroxyapatite, the mineral component of bone. Once bound to the bone surface, bisphosphonates are taken up by osteoclasts during resorption. Inside the osteoclast, nitrogen-containing bisphosphonates inhibit farnesyl pyrophosphate synthase in the mevalonate pathway, disrupting cytoskeletal organization, blocking formation of the ruffled border required for resorption, and inducing osteoclast apoptosis. The net effect is potent reduction in bone resorption, shifting the remodeling balance toward formation and increasing BMD over time.
Oral bisphosphonates: alendronate 70 mg once weekly (treatment) or 35 mg weekly (prevention); risedronate 35 mg weekly or 150 mg monthly; ibandronate 150 mg monthly orally or 3 mg quarterly IV (with weaker evidence for hip-fracture reduction). Intravenous zoledronic acid is dosed at 5 mg IV once yearly, is the most potent bisphosphonate, and offers perfect adherence because it is given by infusion.
The administration requirements for oral bisphosphonates are tested directly. Bioavailability is poor (only 1–3% absorbed). To maximize absorption and minimize esophageal injury, the medication must be taken first thing in the morning on an empty stomach, swallowed with a full glass of plain water (not coffee, juice, or mineral water), and the patient must remain upright (sitting or standing) for at least 30 minutes. No food, drink, or other medications are permitted during that 30-minute window. Calcium supplements bind bisphosphonates and must be separated from the dose.
Bisphosphonates reduce vertebral fractures by 40–70% and hip fractures by 40–50%; non-vertebral fractures are also reduced. The benefit begins within the first year.
A critical pharmacologic distinction: bisphosphonates are anti-resorptive (they slow resorption rather than build new bone). The BMD increase reflects filling-in of remodeling spaces and continued secondary mineralization. This contrasts with anabolic agents (teriparatide, romosozumab) that directly stimulate osteoblast activity and new bone formation.
Renal contraindications are testable. Bisphosphonates are renally excreted and accumulate in severe renal impairment. They are contraindicated when the creatinine clearance (CrCl) is below 30–35 mL/min depending on agent. In a patient with chronic kidney disease (CKD) and osteoporosis, denosumab becomes the preferred anti-resorptive.
The adverse effects are heavily tested. Upper gastrointestinal effects (esophagitis, esophageal erosions and ulcerations) are the most common adverse effects of oral bisphosphonates and are minimized by strict adherence to the upright-with-water protocol. Oral bisphosphonates are contraindicated in patients with esophageal disorders that delay emptying (achalasia, esophageal stricture) and in patients who cannot remain upright for 30 minutes.
Osteonecrosis of the jaw (ONJ) is rare but serious. It presents as exposed, nonhealing bone in the oral cavity, typically after a dental extraction or invasive dental procedure. The risk is much higher with high-dose IV bisphosphonate use in cancer patients than with osteoporosis-dose therapy. Dental evaluation and completion of necessary invasive dental work are recommended before starting therapy.
Atypical femoral fractures are associated with prolonged bisphosphonate use, typically after 5 or more years. They occur in the subtrochanteric region or femoral shaft (not the typical intertrochanteric or femoral neck location of osteoporotic hip fractures). The fractures are transverse or short oblique, occur with minimal or no trauma, and are often preceded by prodromal thigh or groin pain for weeks to months. They may be bilateral; if one occurs, image the contralateral femur. The proposed mechanism is excessive suppression of bone remodeling, which prevents repair of microdamage and allows stress fractures to propagate. Atypical femoral fractures drive the drug-holiday recommendation.
The drug holiday is a critical board topic. Bisphosphonates bind tightly to bone and continue to exert anti-resorptive effects long after the medication is stopped. The general recommendation is a drug holiday after 5 years of oral bisphosphonate therapy or 3 years of IV zoledronic acid therapy. During the holiday, BMD and fracture risk are reassessed periodically; treatment is resumed if BMD declines significantly or a new fracture occurs. Holiday duration is typically 2–3 years for prior oral users and 3–6 years for prior zoledronic acid users, reflecting the longer skeletal half-life of the IV agent.
An acute-phase reaction with flu-like symptoms (fever, myalgia, arthralgia) can occur within 24–72 hours of IV bisphosphonate infusion, particularly with the first dose of zoledronic acid. It occurs in roughly 30% of first-dose patients, is caused by inflammatory cytokine release from gamma-delta T cells, and typically resolves within 48–72 hours. Pretreatment with acetaminophen reduces severity, and the incidence diminishes with subsequent infusions.
Hypocalcemia can follow bisphosphonate administration when vitamin D is deficient, because abrupt resorption suppression removes a calcium flux source. Vitamin D and calcium should be replete (25-OH-D >30 ng/mL) before initiating any anti-resorptive.

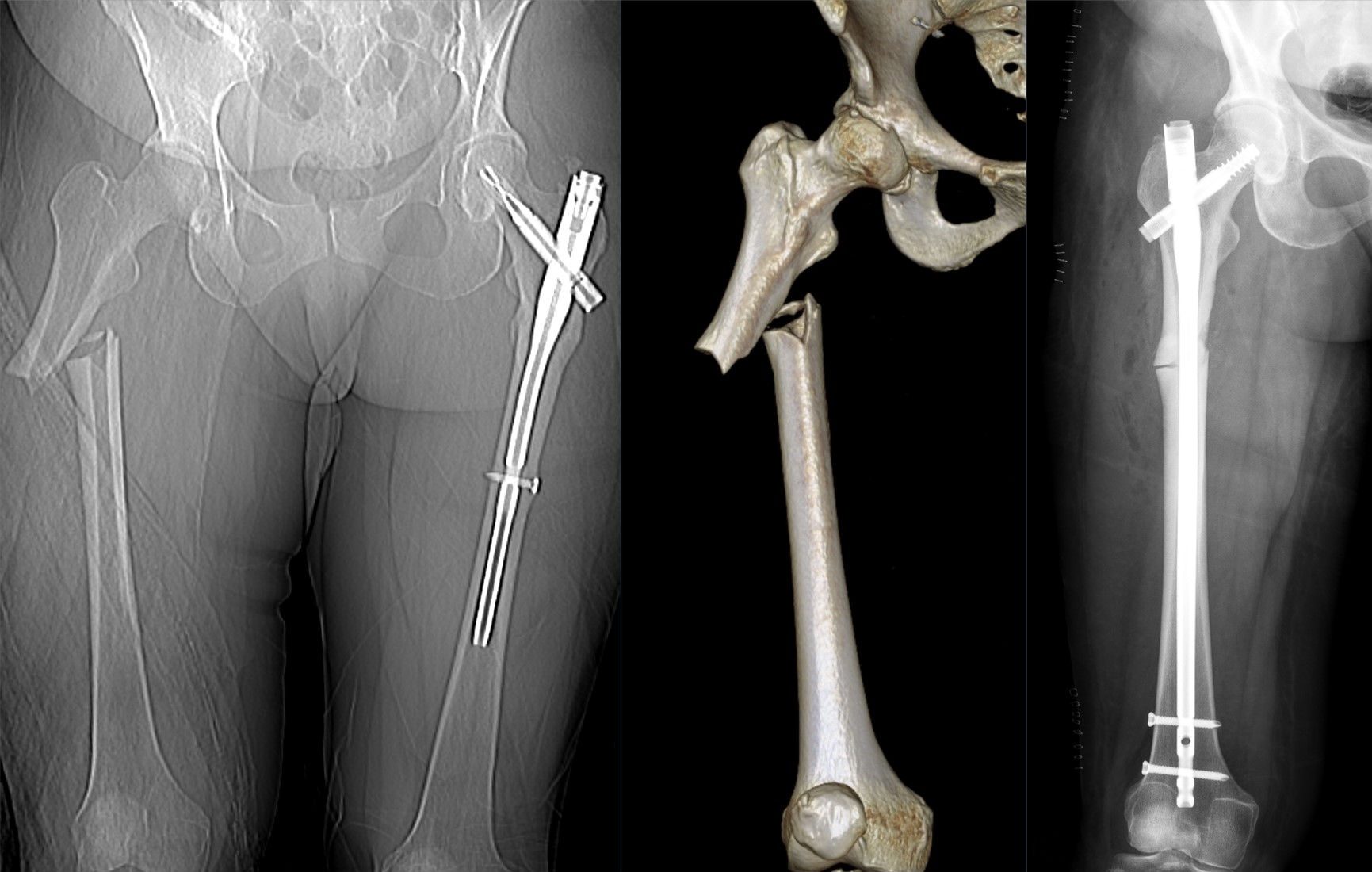
Source: Hellerhoff, Wikimedia Commons, CC BY-SA 4.0

Source: Mikael Häggström MD, Wikimedia Commons, CC0 (Public Domain)
High Yield — Bisphosphonates

- Mechanism: bind hydroxyapatite → enter osteoclasts → inhibit mevalonate-pathway farnesyl pyrophosphate synthase → osteoclast apoptosis.
- Oral discipline: empty stomach, plain water, upright 30 min, no food/drink/meds in window, separate from calcium.
- Bioavailability of oral form ≈ 1–3%.
- Major adverse effects: esophagitis (oral), atypical subtrochanteric/diaphyseal femur fracture with prodromal thigh pain after ≥5 years, ONJ, acute-phase reaction (first IV dose), hypocalcemia when vitamin D deficient.
- Drug holiday: 5 yr oral, 3 yr IV; reassess and restart if BMD drops or fracture occurs.
- Renal contraindication at CrCl <30–35 mL/min; switch to denosumab.
- Replete vitamin D (>30 ng/mL) before starting.
Board Trap — “Take with orange juice for the calcium”

A patient asks if she can take her weekly alendronate with orange juice to make it easier on the stomach. The trap is to say yes. Oral bisphosphonates require plain water only; juice (and coffee, mineral water, milk) impairs absorption. The remainder of the protocol is empty stomach, full glass of water, sitting or standing for 30 minutes, no food or other medications in that window, and calcium separated from the dose. The protocol is tested as a recognition item: any deviation reduces absorption from the already poor 1–3% bioavailability or raises esophagitis risk.
Without farnesyl pyrophosphate synthase, the osteoclast cannot maintain that ruffled border. It loses its grip, its internal structure collapses, and this disruption is so profound that it induces apoptosis. The net effect of killing off the osteoclasts is a highly potent anti-resorptive state.
— MSK-24 podcast, ~04:47