MSK · EP 25 · PROCEDURES
Before You Listen
Episode Setup
- Topic in one line: the procedural toolbox of physiatry: musculoskeletal ultrasound transducer selection and tissue echotextures, anisotropy as the headline artifact, dynamic versus static assessment, ultrasound-guided injection, synovial fluid analysis with the cell-count thresholds and crystal birefringence, joint and bursa injection approaches, corticosteroid and local-anesthetic selection, the artery of Adamkiewicz catastrophe in transforaminal epidural steroid injection, sacroiliac joint diagnostic blocks, the stellate ganglion block and Horner sign, and botulinum toxin and chemical neurolysis for spasticity.
- Prerequisites: sectional musculoskeletal anatomy, the basic concept of ultrasound (sound waves and reflection at tissue interfaces), the SNARE-mediated acetylcholine release at the neuromuscular junction, and the lumbar and cervical foraminal anatomy.
- Runtime: 1 hour 2 minutes.
Vignette. A 58-year-old woman with right-sided cervical radiculopathy that has not responded to 8 weeks of physical therapy is referred for a transforaminal epidural steroid injection (TFESI) at the C6 nerve root. She has a history of supraventricular tachycardia treated with a beta-blocker, no prior local-anesthetic exposure, and a body mass index (BMI) of 27. The proceduralist plans the injection under fluoroscopic guidance. As the needle approaches the foramen and contrast is injected before steroid, the contrast briefly outlines a vascular blush rather than the expected nerve-root pattern.
What is the catastrophic complication being prevented in that moment, what is the anatomic vessel that anchors this risk, why is the choice of corticosteroid (particulate versus non-particulate) one of the highest-yield concepts in the entire procedural block, and what should the proceduralist do next? In a parallel scenario where a different patient develops perioral numbness, tinnitus, agitation, and ventricular arrhythmia after a peripheral injection of bupivacaine, what is the diagnosis and what is the definitive antidote?
(Answer at the end of this chapter)
Section 1: Ultrasound Physics, Transducer Selection, and Tissue Echotextures
Bottom line: musculoskeletal ultrasound uses high-frequency (10–18 megahertz) linear transducers for superficial structures with excellent resolution but limited penetration, and lower-frequency (2–6 megahertz) curvilinear transducers for deep structures like the hip; tendons are hyperechoic and fibrillar, muscle is hypoechoic with pennate architecture, nerves show a honeycomb pattern in short axis, bone cortex is hyperechoic with posterior shadowing, and fluid is anechoic with posterior enhancement; the highest-yield artifact is anisotropy, the angle-dependent loss of echogenicity that makes a normal tendon look hypoechoic when the beam is not perpendicular.
Musculoskeletal ultrasound is now an essential PM&R tool, and the boards test its physics, transducer selection, tissue appearance, and artifacts.
Transducer selection is determined by target depth. High-frequency linear transducers (10–18 MHz) are the workhorse, providing excellent spatial resolution for superficial structures (tendons, ligaments, superficial nerves, extremity joints) with penetration limited to ~4–6 cm. Curvilinear (convex) transducers at lower frequencies (2–6 MHz) provide greater penetration at the cost of resolution for deep structures (hip joint, sciatic nerve in the gluteal region, deep pelvic targets). Hockey-stick transducers are small-footprint high-frequency probes for fingers, toes, and small targets. The principle: higher frequency = better resolution, less penetration; lower frequency = more penetration, less resolution.
Tissue echogenicity is the brightness on ultrasound. Hyperechoic structures appear bright. Bone cortex produces a bright linear echo with posterior acoustic shadowing. Tendons are hyperechoic with fibrillar echotexture (parallel bright lines in long axis, organized collagen bundles). Muscle is hypoechoic with pennate echotexture in long axis (obliquely oriented hypoechoic bundles separated by hyperechoic septa) and a stippled “starry sky” pattern in short axis. Articular cartilage is hypoechoic to anechoic, a smooth dark layer between hyperechoic bone and overlying soft tissue. Ligaments are hyperechoic and tightly fibrillar (more compact than tendon, a high-yield distinction). Nerves show a honeycomb pattern in short axis (small hypoechoic fascicles surrounded by hyperechoic epineurium) and parallel hypoechoic fascicles in long axis; nerves are less echogenic than tendons and show less prominent anisotropy.
Fluid is anechoic when simple, hypoechoic with internal echoes when complex (hemorrhage, debris, infection). Pathology patterns: tendinosis = tendon thickening with loss of fibrillar echotexture; partial tear = focal hypoechoic defect; full-thickness tear = discontinuity with retraction. Bursitis appears as distension of a bursa with anechoic/hypoechoic fluid (subacromial-subdeltoid distension >2 mm is abnormal). Synovitis appears as hypoechoic thickening of the synovial lining; power Doppler shows increased vascularity correlating with active inflammation. Inflammatory erosions in rheumatoid arthritis appear as cortical irregularities at joint margins, often visible on ultrasound before plain radiographs show them.


Source: Harrison Keely, Wikimedia Commons, CC BY 4.0

Source: Kalumet & Dirk Hünniger, Wikimedia Commons, CC BY-SA 3.0 / GFDL
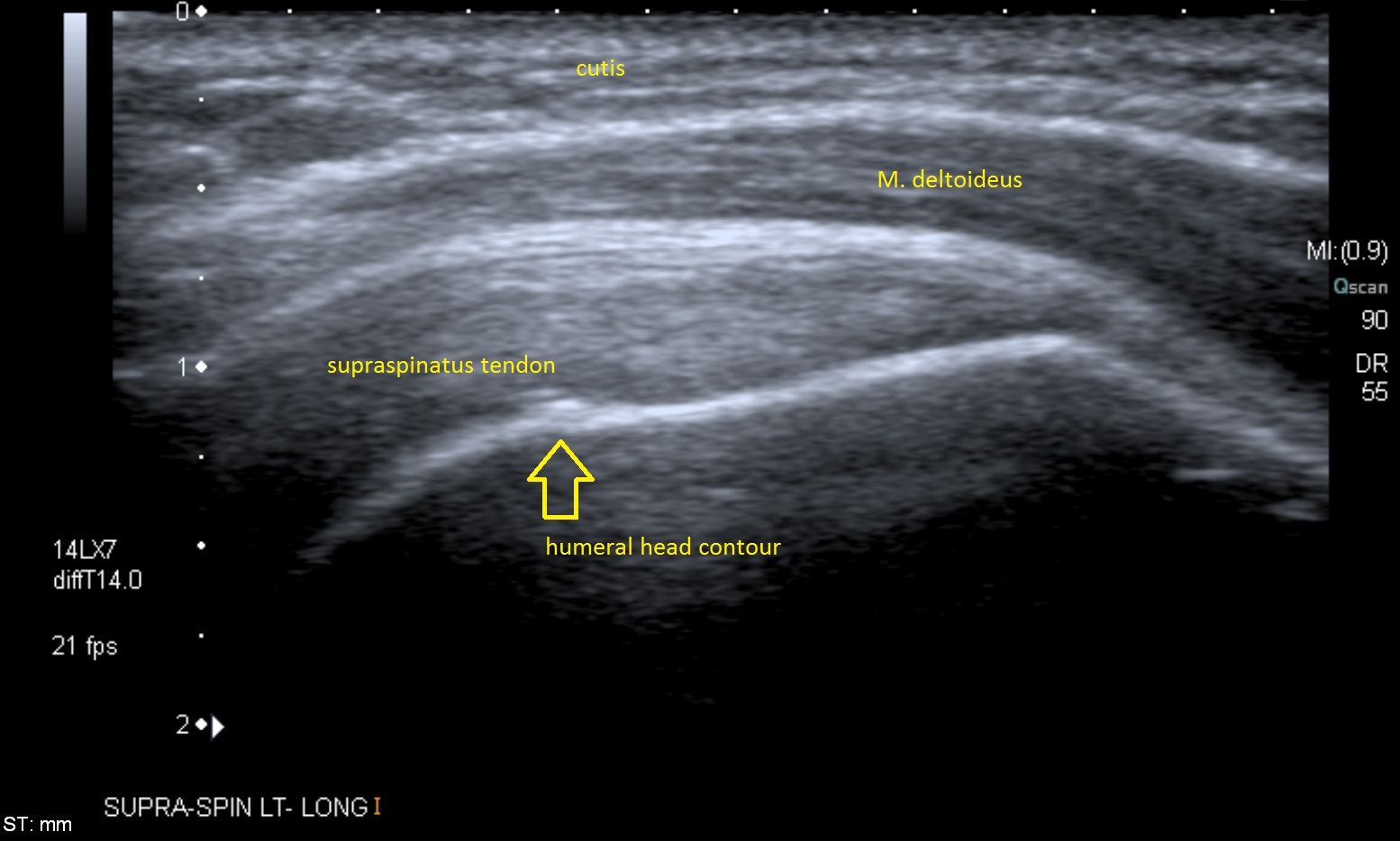
Source: RSatUSZ (PACS UniversitätsSpital Zürich), Wikimedia Commons, CC BY-SA 4.0 / GFDL
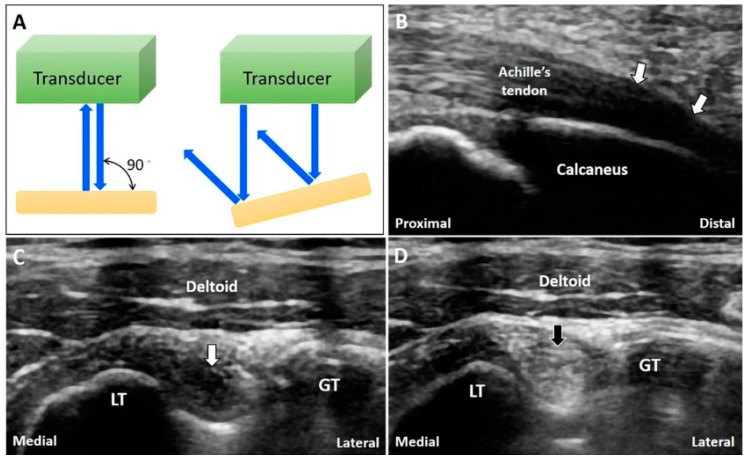
Source: Draghi F et al., Diagnostics 2020;10(9):645, CC BY 4.0
High Yield — Ultrasound physics and tissue patterns
- Linear high-freq (10–18 MHz) = superficial; curvilinear low-freq (2–6 MHz) = deep.
- Higher frequency: better resolution, less penetration. Lower frequency: more penetration, less resolution.
- Hyperechoic + posterior shadowing = bone cortex.
- Fibrillar hyperechoic in long axis = tendon.
- Pennate hypoechoic / starry sky = muscle.
- Honeycomb in short axis = nerve (less echogenic, less anisotropy than tendon).
- Anechoic + posterior enhancement = fluid (cyst, effusion, bursitis).
- Power Doppler signal in synovium = active inflammation.
- Erosions on ultrasound often precede plain-radiograph appearance in inflammatory arthritis.