MSK · EP 26 · NERVE
Before You Listen
Episode Setup
- Topic in one line: the framework that ties peripheral nerve trauma to electrodiagnosis: the Seddon and Sunderland classifications, the Wallerian degeneration timeline that determines when an electrodiagnostic (EDX) study can detect what, the EDX signatures of demyelination versus axon loss, the one-millimeter-per-day regeneration rate, and the EDX-musculoskeletal correlation for the high-yield compressive nerve injuries (radial, peroneal, brachial plexus, axillary, median, ulnar, tibial, femoral, sciatic).
- Prerequisites: EDX series basics (the dorsal root ganglion (DRG) rule, motor unit physiology, conduction velocity and amplitude conventions from EDX-01), brachial plexus and lumbosacral plexus anatomy from MSK-03 and MSK-08.
- Runtime: 1 hour 5 minutes.
Vignette. A 38-year-old man falls asleep on a bar stool with his right arm draped over the back of the seat. He wakes seven hours later unable to extend his wrist or fingers, with numbness over the dorsum of the hand in the first dorsal web space. Triceps strength is preserved. He is referred for an electrodiagnostic study performed three days after the event. The radial compound muscle action potential (CMAP) recorded from extensor indicis proprius is normal with stimulation at the forearm but reduced with stimulation above the spiral groove. The radial sensory nerve action potential (SNAP) at the snuffbox is normal. Needle examination of the radial-innervated forearm extensors shows reduced recruitment but no fibrillation potentials.
Where is the lesion, what explains the absence of fibrillation potentials at day three, what Seddon and Sunderland grade fits the day-three findings, what is the optimal timing for a comprehensive study, and what is the expected recovery timeline?
(Answer at the end of this chapter)
Section 1: Seddon and Sunderland — The Two Classification Systems
Bottom line: the Seddon classification (1943) sorts nerve injury into three grades based on which structures are disrupted (neurapraxia, axonotmesis, neurotmesis) and the Sunderland classification (1951) refines axonotmesis into three sub-grades based on which connective tissue layer is breached; neurapraxia is pure focal demyelination with conduction block and no Wallerian degeneration; axonotmesis disrupts the axon while preserving the endoneurial tube, allowing regeneration at one millimeter per day; neurotmesis is complete transection that requires surgical repair because the connective tissue scaffold guiding regrowth is gone.
The Seddon classification (Herbert Seddon, 1943) sorts peripheral nerve injuries into three categories based on the degree of structural disruption: neurapraxia, axonotmesis, and neurotmesis. The Sunderland classification (Sydney Sunderland, 1951) refines this into a five-grade system that maps injury onto the three concentric connective tissue layers (endoneurium, perineurium, epineurium). The two systems are complementary: Sunderland grade 1 equals neurapraxia, grade 2 equals classical axonotmesis, grades 3 and 4 are progressively more disrupted axonotmesis, and grade 5 equals neurotmesis.
Neurapraxia is a focal demyelinating lesion with the axon entirely intact through the lesion. Because the axon is not severed, no Wallerian degeneration occurs distally. The hallmark electrodiagnostic finding is conduction block: stimulation distal to the lesion produces a normal CMAP, while stimulation proximal produces a reduced or absent response. Needle electromyography (EMG) shows no fibrillation potentials, because the muscle is not denervated. Motor unit potentials are normal in morphology, although recruitment is reduced because fewer motor units are accessible across the block. Recovery is full and occurs over weeks to a few months as Schwann cells remyelinate the affected internode. Because remyelination is faster than axonal regeneration, recovery is often abrupt: once the myelin is repaired, conduction is restored.
Axonotmesis disrupts the axon while the endoneurium remains intact. Wallerian degeneration proceeds distal to the lesion over the first one to two weeks. Because the endoneurial tube is preserved, regenerating axon sprouts have a physical scaffold guiding them back to their original targets. On nerve conduction studies (NCS), the distal CMAP amplitude falls first (begins by day three to five, complete by day seven to nine) and the SNAP falls slightly later (begins around day six, complete by day ten to eleven). Once Wallerian degeneration is complete, fibrillation potentials and positive sharp waves appear on needle EMG. Recovery proceeds through axonal regeneration at approximately one millimeter per day (about one inch per month). Time to recovery is directly proportional to the distance from the lesion to the target muscle.
Neurotmesis is complete disruption of the nerve including all connective tissue layers. Wallerian degeneration occurs as in axonotmesis, but the endoneurial scaffold is gone. Spontaneous recovery does not occur; regenerating axons instead form a disorganized neuroma at the proximal stump. Surgical repair is required. Importantly, electrodiagnostic studies cannot reliably distinguish neurotmesis from severe axonotmesis in the acute window: both show identical complete distal axon loss with absent CMAP and SNAP, dense fibrillations, and absent voluntary recruitment. The differentiation comes from clinical course: axonotmesis shows an advancing Tinel sign and serial EMG signs of reinnervation; neurotmesis does not.
The Sunderland system decomposes axonal injury by which connective tissue layer is disrupted. Grade 1 = neurapraxia (myelin only). Grade 2 = classical axonotmesis (endoneurium intact; good recovery). Grade 3 disrupts the endoneurium; regenerating axons may enter wrong tubes, producing misdirected reinnervation with synkinesis (simultaneous contraction of muscles that should not co-contract). Grade 4 leaves only the epineurium intact; a neuroma-in-continuity typically forms and surgery is usually required. Grade 5 = neurotmesis (complete transection). A Mackinnon grade 6 describes a mixed injury in which different fascicles sustain different grades; this is the most common real-world pattern and explains why partial recovery with persistent deficits is so frequently seen.

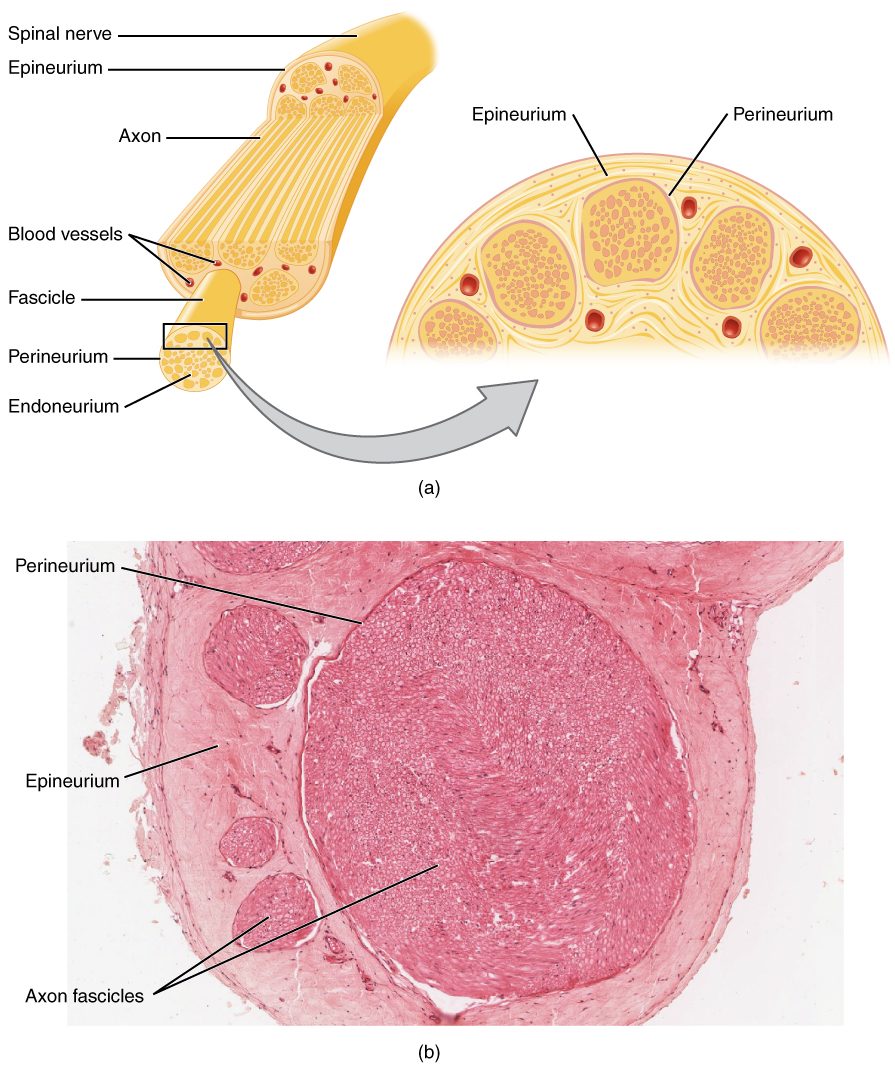
Source: OpenStax Anatomy & Physiology (Fig. 13.4 / 1319), CC BY 4.0
High Yield — Seddon and Sunderland
- Neurapraxia (Sunderland 1) = focal demyelination only; axon intact; no Wallerian degeneration; conduction block on NCS; no fibrillations on EMG; full recovery in weeks to a few months.
- Axonotmesis (Sunderland 2) = axon disrupted; endoneurium intact; Wallerian degeneration; fibrillations on the standard timeline; regeneration at 1 mm/day along the endoneurial tube.
- Sunderland 3 = endoneurium disrupted; misdirected reinnervation; synkinesis possible.
- Sunderland 4 = only epineurium intact; neuroma-in-continuity; surgery typically required.
- Neurotmesis (Sunderland 5) = complete transection; no spontaneous recovery; surgical repair required.
- Mackinnon grade 6 = mixed injury (different fascicles, different grades); the most common clinical reality.
- EDX cannot distinguish Sunderland 2-5 in the acute period; clinical course, advancing Tinel sign, and serial EDX over months are required.
Mnemonic — “Mile Markers from 1 to 5”

Walk the mnemonic from outside-in on the connective tissue: 1 = myelin only (neurapraxia); 2 = + axon (axonotmesis with endoneurium spared); 3 = + endoneurium (misdirected reinnervation); 4 = + perineurium (only epineurium left, neuroma-in-continuity); 5 = + epineurium (complete transection, neurotmesis). Each step inward predicts a worse recovery.
Seddon is a bit like looking at the nervous system with a magnifying glass. It gives us the big picture. The Sunderland classification system, which came slightly later, zooms in with a high-powered microscope. Sunderland grade one strictly equals Seddon’s neuropraxia, and Sunderland grade two strictly equals Seddon’s axonotmesis in its purest form — the axon breaks, Wallerian degeneration occurs, but the innermost layer, the endoneurium, remains entirely intact.
— MSK-26 podcast, ~18:02