REHAB · EP 08 · OUTCOMES
Before You Listen
Episode Setup
- Topic in one line: the rehabilitation outcome-measurement toolkit, anchored by the World Health Organization (WHO) International Classification of Functioning, Disability and Health (ICF) framework, the Functional Independence Measure (FIM) with its 18 items, 7-level ordinal scoring, and 75/50/25 percent effort breakpoints, the Barthel Index ceiling effect, the Glasgow Coma Scale (GCS) “minimum is 3, not zero” rule, the Rancho Los Amigos cognitive-recovery levels, the National Institutes of Health Stroke Scale (NIHSS) posterior-circulation blind spot, the modified Rankin Scale (mRS), the American Spinal Injury Association Impairment Scale (AIS) A-E grades, the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) cutoffs, the Berg/Tinetti/Timed Up and Go (TUG) fall-risk thresholds, the Coma Recovery Scale-Revised (CRS-R) for disorders of consciousness, the inpatient rehabilitation facility (IRF) 60% rule and 3-hour rule, and the psychometric vocabulary of reliability, validity, responsiveness, and minimal clinically important difference (MCID).
- Prerequisites: familiarity with manual muscle testing 0-5, basic neuroanatomy of the corticospinal tract, the upper-versus-lower-motor-neuron distinction, and the spinal cord injury concepts of motor and sensory levels.
- Runtime: 1 hour 8 minutes.
Vignette. A 67-year-old woman is admitted to your inpatient rehabilitation facility (IRF) ten days after a left middle cerebral artery ischemic stroke. Acute hospital National Institutes of Health Stroke Scale (NIHSS) was 14. On admission her Glasgow Coma Scale (GCS) is 14 (eye 4, verbal 4, motor 6), Functional Independence Measure (FIM) total is 52 (motor 32, cognitive 20), and Berg Balance Scale is 22. She requires moderate assistance to transfer (the therapist provides about 40 percent of the effort), maximal assistance to dress her lower body, and supervision for eating after setup. Her right upper extremity is flaccid; her right lower extremity has trace knee flexion. She follows simple commands inconsistently and confuses staff names.
What FIM scores correspond to her transfer, lower-extremity dressing, and eating performance, what Brunnstrom stage describes her right upper extremity, what Berg threshold has she crossed for fall risk, what Rancho Los Amigos level matches her cognitive picture, and which IRF Medicare rules govern whether she can stay on your unit?
(Answer at the end of this chapter)
Section 1: The ICF Framework, ADL/IADL Hierarchy, and Measurement Concepts
Bottom line: the World Health Organization International Classification of Functioning, Disability and Health (ICF) reframes disability as the interaction of body functions and structures, activities, and participation, modified by environmental and personal contextual factors; activities of daily living (ADLs) are the six basic self-care tasks (bathing, dressing, toileting, transferring, continence, feeding) the Katz Index tracks in their hierarchical loss-and-recovery sequence, while instrumental activities of daily living (IADLs) are the eight community-living tasks (telephone, shopping, food prep, housekeeping, laundry, transportation, medication, finances) Lawton and Brody catalogued; rehabilitation outcome data is almost entirely ordinal, which means medians and nonparametric tests are the statistically correct analytic tools and the routine “mean FIM score” reported in research is a convenient violation that the boards will test.
The WHO International Classification of Functioning, Disability and Health (ICF), ratified in 2001, is the conceptual scaffold that organizes every other tool in this chapter. The ICF replaces the older impairment-disability-handicap model with a biopsychosocial framework. Body functions and structures describe physiologic and anatomic substrate (a hemiparetic limb, a damaged brain). Activity describes what the person can do at the individual level (transfer, walk, dress). Participation describes engagement in life roles (return to work, community mobility, parenting). These three domains are modified by contextual factors: environmental (ramps, attendant care, attitudes of others) and personal (age, coping style, education). The ICF replaces “handicap” with “participation restriction” deliberately, because where impairment translates into disability depends almost entirely on environment.
A C6 tetraplegic with a power wheelchair, accessible housing, and a desk job has minimal participation restriction despite substantial impairment, while the same impairment in a third-floor walk-up apartment produces total participation restriction. Outcome measurement must capture all three levels: impairment scales (Modified Ashworth Scale (MAS), manual muscle testing) at the body level, FIM and Barthel at the activity level, and the Craig Handicap Assessment and Reporting Technique (CHART) at the participation level.
Activities of daily living (ADLs) are the six basic self-care tasks the Katz Index codified in 1963: bathing, dressing, toileting, transferring, continence, and feeding. Katz observed that these are lost in fixed hierarchical order during functional decline (bathing first, feeding last) and recovered in reverse order. This makes the Katz Index uniquely informative for tracking dementia trajectory and post-stroke recovery sequence.
Instrumental activities of daily living (IADLs) are the eight community-living tasks Lawton and Brody added in 1969: telephone, shopping, food preparation, housekeeping, laundry, transportation, medication management, and finances. IADLs are higher-order than ADLs and are typically lost earlier in cognitive decline.

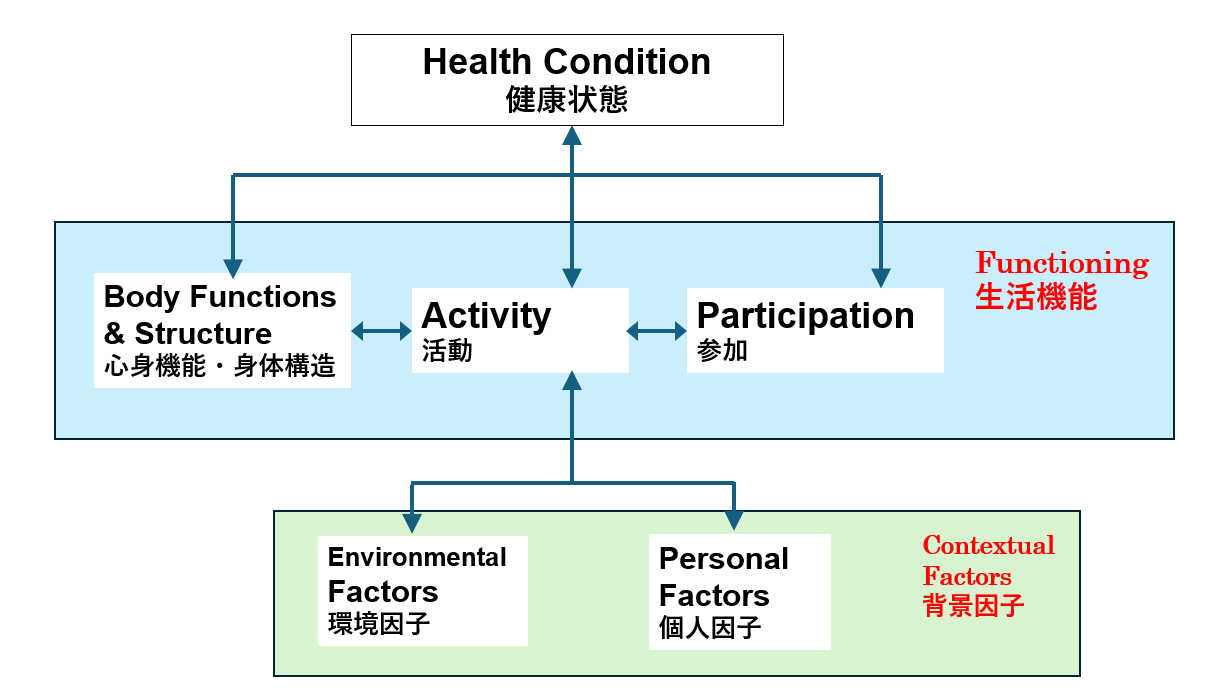
Source: World Health Organization, Wikimedia Commons, CC BY 3.0
The fundamental measurement-concept distinction the boards test is the four levels of measurement: nominal (unordered categories such as diagnosis or blood type), ordinal (ranked but unequal intervals: FIM, MAS, manual muscle testing, mRS), interval (equal intervals, no true zero, such as temperature in Celsius), and ratio (equal intervals with a true zero: weight, distance, time, range of motion in degrees). Nearly every rehabilitation outcome scale produces ordinal data. The clinical implication is that the appropriate central-tendency measure is the median (not the mean), and the appropriate analytic tools are nonparametric tests (Mann-Whitney U, Wilcoxon signed-rank, Kruskal-Wallis) rather than parametric tests (t-test, analysis of variance). Despite this, mean FIM scores and parametric tests on FIM data fill the rehabilitation literature; the board answer is that ordinal data calls for nonparametric methods.
The psychometric vocabulary is also board-testable. Reliability is consistency: inter-rater reliability (agreement between examiners; kappa or intraclass correlation coefficient) and test-retest reliability (consistency over time). Validity is whether the instrument measures what it claims: content (items represent the construct), criterion (compared to a gold standard), and construct (scale behaves as theory predicts). Responsiveness is the ability to detect meaningful change. The minimal clinically important difference (MCID) is the smallest change considered worthwhile; established values include approximately 22 points for total FIM after stroke and approximately 50 meters for the 6-minute walk test in chronic obstructive pulmonary disease.
High Yield — ICF, ADLs, and measurement levels

- ICF triad: body functions/structures + activity + participation, modified by environmental and personal factors. Environment is the decisive modifier.
- ADLs (Katz, 6 items): bathing, dressing, toileting, transferring, continence, feeding. Lost bathing-first, feeding-last; recovered in reverse.
- IADLs (Lawton-Brody, 8 items): telephone, shopping, food prep, housekeeping, laundry, transportation, medication, finances. Higher-order than ADLs; lost earlier in cognitive decline.
- Levels of measurement: nominal, ordinal, interval, ratio. Almost every rehabilitation scale is ordinal.
- Ordinal data analysis: report median (not mean) and use nonparametric tests (Mann-Whitney U, Wilcoxon).
- Reliability: inter-rater (kappa, intraclass correlation coefficient) and test-retest. Validity: content, criterion, construct.
- Responsiveness and MCID: the smallest change the patient considers worthwhile; FIM stroke MCID approximately 22 points.