BASIC · EP 07 · NERVE
Before You Listen
Episode Setup
- Topic in one line: the peripheral nerve injury framework that runs through every electrodiagnostic, traumatic, and rehabilitation question: peripheral nerve microanatomy (axon, Schwann cell, endoneurium, perineurium, epineurium); the Seddon three-tier (neurapraxia, axonotmesis, neurotmesis) and Sunderland five-grade (plus Mackinnon Grade VI) classifications mapped to the connective tissue layers; the Wallerian degeneration timeline (NMJ failure at days 3-5, motor axons inexcitable at days 5-7, sensory at days 10-11); the bands of Büngner formed by dedifferentiated Schwann cells that guide axonal regeneration at approximately 1 mm per day; the 12-18 month motor end-plate viability window; and the surgical reconstruction options (primary neurorrhaphy, sural nerve grafting, the Oberlin nerve transfer).
- Prerequisites: comfort with basic neuron anatomy, the difference between motor and sensory fibers, and the standard electrodiagnostic vocabulary (compound muscle action potential (CMAP), sensory nerve action potential (SNAP), motor unit action potential (MUAP), fibrillation potentials, positive sharp waves) introduced earlier in the BASIC series.
- Runtime: approximately 30 minutes for Part 1.
- Scope boundary: Part 1 builds the framework: anatomy, classification, the Wallerian timeline, regeneration biology, and the surgical reconstruction menu. Part 2 turns that framework into bedside diagnosis. It walks the named clinical syndromes (Saturday night palsy, anterior and posterior interosseous neuropathies, scapular winging, Erb-Duchenne and Klumpke palsies, common peroneal at the fibular head), the electrodiagnostic distinction of peroneal neuropathy from L5 radiculopathy, the modulators of recovery, and the rehabilitation prescription (splinting, range of motion, neuropathic pain, sensory re-education).
Vignette. A 32-year-old man sustains a sharp laceration to the medial elbow from a glass injury, with immediate numbness in the small finger and the ulnar half of the ring finger and weakness of finger abduction and adduction. He is taken to the emergency department where the wound is irrigated and closed; ulnar nerve continuity is not formally explored. Two weeks later he is referred for electrodiagnostic evaluation. Distal stimulation of the ulnar nerve at the wrist generates a CMAP amplitude of 0.5 mV (reference 8 mV) with no SNAP recordable from the small finger. Needle examination of the abductor digiti minimi shows reduced recruitment with no fibrillations or positive sharp waves yet visible.
What Seddon and Sunderland grade does this presentation suggest, what is the optimal timing for the next electrodiagnostic study and what new findings should be expected at that time, what is the expected timeline for axonal regeneration to reach the abductor digiti minimi if the injury is axonotmesis with intact endoneurium, and what surgical options exist if regeneration cannot beat the motor end-plate viability window?
(Answer at the end of this chapter)
Section 1: Peripheral Nerve Anatomy and the Seddon-Sunderland Classification
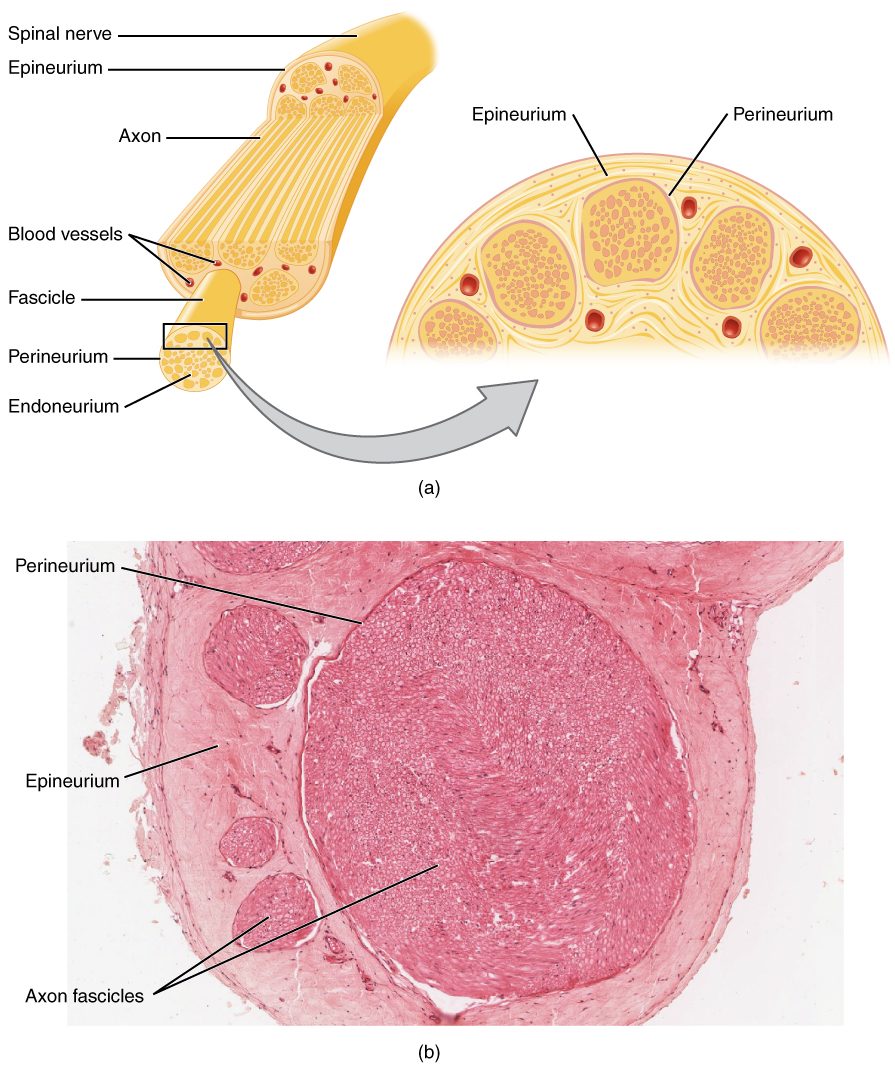
Bottom line: the peripheral nerve is a layered composite of axons wrapped in three concentric connective tissue sheaths (endoneurium around individual fibers, perineurium around fascicles, epineurium around the whole trunk), and the integrity of each successive layer determines the grade of injury and the prognosis for recovery. Seddon (1943) distinguishes neurapraxia (focal demyelination, conduction block, no Wallerian degeneration, full recovery in days to 12 weeks), axonotmesis (axon disrupted, endoneurium intact, Wallerian degeneration occurs, regeneration along the preserved tube at 1 mm per day), and neurotmesis (complete transection, surgical repair required). Sunderland (1951) maps that into five grades anchored to the connective tissue layers (Grade I myelin only, Grade II adds axon, Grade III adds endoneurium, Grade IV adds perineurium, Grade V is complete transection), and Mackinnon added Grade VI for the mixed injuries that dominate real-world trauma. The single most useful prognostic question is whether the endoneurium is intact.
The peripheral nerve behaves like a layered fiber-optic cable. The axon is the conducting unit. Myelinated axons are wrapped 1:1 by Schwann cells in 1-mm internodes separated by nodes of Ranvier, where voltage-gated sodium channels regenerate the action potential by saltatory conduction. Unmyelinated axons are grouped together in Remak bundles. Three concentric connective tissue layers then envelop the axons. The endoneurium wraps each individual nerve fiber and provides both the blood-nerve barrier and the regeneration scaffold that determines whether a regenerating axon finds its original target. The perineurium bundles axons into fascicles. It is the strongest connective layer per unit thickness and provides the tensile strength and diffusion barrier that protect the fascicle. The epineurium encloses the whole nerve trunk, carrying the vasa nervorum and providing the mechanical cushioning that lets the nerve glide across joints.
The integrity of each layer determines the grade of injury and the prognosis for recovery. Two complementary classification systems formalize this, and both still appear on every board examination.
Seddon (1943) proposed the three-tier system that remains the bedside vocabulary. Neurapraxia is focal demyelination with axonal continuity preserved. The signal cannot pass the lesion site, but the wire is structurally whole. There is no Wallerian degeneration. The CMAP is preserved with stimulation distal to the lesion and blocked across the injury site. There are no fibrillations on EMG because the muscle fibers are still attached to intact axons. Full recovery occurs in days to 12 weeks as the local Schwann cells repair the bruised myelin. Saturday night palsy (radial nerve compression at the spiral groove from draping the arm over a chair) is the prototype. Axonotmesis disrupts the axon but preserves the endoneurium. Wallerian degeneration occurs distally, the CMAP and SNAP fall, fibrillations emerge by 2-3 weeks, and regeneration follows the preserved endoneurial tube at approximately 1 mm per day to its original target with generally good functional recovery if the distance is short. Neurotmesis is complete transection through the axon and every connective tissue layer. Spontaneous recovery is not possible. Surgical repair is mandatory, and functional outcomes remain limited because axonal misdirection is inevitable once the endoneurial tubes are disrupted.
Sunderland (1951) expanded Seddon into five grades anchored to the specific connective tissue layers disrupted, providing the granularity needed for surgical decision-making. Mackinnon added Grade VI to capture the mixed-grade injuries that dominate real-world trauma.

Grade I (neurapraxia) is segmental demyelination with conduction block; recovery by remyelination is complete within 12 weeks. Grade II (axonotmesis) disrupts the axon while preserving the endoneurial basal lamina tube; Wallerian degeneration occurs distally, and the regenerating axon advances along the preserved tube at 1 mm per day with generally good functional recovery. Grade III disrupts axon and endoneurium with perineurium intact; fascicular architecture is preserved at the macroscopic level, but intrafascicular fibrosis impedes regeneration and allows misdirection within the same fascicle. The image is a multi-lane highway with the painted lane lines erased: motor axons may grow down sensory tubes and vice versa. Grade IV extends disruption to the perineurium; the nerve may look grossly intact externally because the epineurial sheath remains, but the interior is a chaotic mess of scar and misdirected sprouts. Intraoperative nerve action potential (NAP) testing distinguishes Grade III from Grade IV in surgery. Grade V is complete transection, identical to Seddon’s neurotmesis. Grade VI is the Mackinnon addition for mixed injuries with different fascicles at different grades; these are common in traction and partial laceration and require intraoperative fascicular assessment, because the surgeon must address the high-grade fascicles without harming lower-grade fascicles recovering spontaneously.
High Yield — Seddon and Sunderland
- Seddon (3 tiers): neurapraxia, axonotmesis, neurotmesis.
- Sunderland (5 grades + Mackinnon VI): I (myelin only) = neurapraxia. II (axon, endoneurium intact) = axonotmesis. III (axon + endoneurium). IV (only epineurium intact). V (complete transection) = neurotmesis. VI (Mackinnon) = mixed injury across fascicles.
- Endoneurium intact (I-II) = good recovery; endoneurium disrupted (III+) = variable to poor because axonal misdirection becomes inevitable once the lane lines are erased.
- Neurapraxia clinical hallmark: CMAP preserved with distal stimulation, blocked across the lesion, no fibrillations on EMG, recovery in days to 12 weeks.
- Axonotmesis clinical hallmark: CMAP and SNAP fall distally, fibrillations appear by 2-3 weeks, regeneration 1 mm/day along the intact endoneurial tube.
- Neurotmesis: requires surgical repair; even with optimal microsurgery, axonal misdirection limits recovery.
Mnemonic — “Endoneurium is the regeneration tube”

The single most useful prognostic question after a peripheral nerve injury is: is the endoneurium intact? Sunderland Grade I and II preserve it, and recovery is generally good. Grade III through V progressively disrupt it, and recovery falls progressively as axonal misdirection becomes inevitable. Memorize the layers from inside out as “E-P-E” (Endoneurium, Perineurium, Epineurium), then count up the Sunderland grades. Each successive grade adds one more layer of disruption.
Think of the endoneurium as the painted lane lines on a multi-lane highway. If those lane lines are completely erased, the cars do not know where to go, even if the concrete barrier on the edge of the highway is intact. Within that intact perineurial wrapper, regenerating axons will start to wander. They can easily miswire into the wrong endoneurial tubes.
— BASIC-07-a podcast, ~15:08