Stroke Rehabilitation Interventions and Functional Assessment
CVA · EP 07 · STROKE
Before You Listen
- Prerequisites: Brunnstrom synergy patterns, the obligatory upper-extremity flexor template and lower-extremity extensor template, and the constraint-induced movement therapy (CIMT) inclusion criteria from CVA-06; the basic structure of the gait cycle (stance and swing phases) and normal swing-phase requirements (~60° knee flexion, ankle dorsiflexion, hip flexion); upper- vs lower-motor-neuron physiology and the corollary that intact peripheral nerves are required to drive surface electrical stimulation; the ankle-foot orthosis (AFO) categories (solid, hinged, posterior leaf spring) introduced in earlier MSK and SCI material.
- Runtime: 28 minutes 1 second.
- Topic in one line: mirror therapy and its mirror-neuron mechanism (Brunnstrom stage 1-2 candidates, also useful for complex regional pain syndrome); functional electrical stimulation (FES) for foot drop via the common peroneal nerve and the intact-lower-motor-neuron requirement; body-weight-supported treadmill training and the Locomotor Experience Applied Post-Stroke (LEAPS) trial showing equivalence with a progressive home exercise program; vagus nerve stimulation (VNS) paired with rehabilitation for chronic upper-extremity deficits ≥9 months post-stroke (FDA-cleared); the hemiplegic gait pattern (circumduction, hip hike, stiff knee from rectus femoris spasticity, equinovarus) with 50-100% energy cost above normal; AFO selection by Brunnstrom stage; the Functional Independence Measure (FIM) (18 items, 7-point ordinal scale, max 126, motor 91, cognitive 35) and FIM efficiency; the Barthel Index (10 items, 0-100); the Fugl-Meyer Assessment (UE max 66, LE max 34); the Berg Balance Scale (<45 = high fall risk); the 10-meter walk test thresholds (0.4 and 0.8 m/s); the Montreal Cognitive Assessment (MoCA) (≥26 normal, +1 if ≤12 years of education); and the World Health Organization (WHO) impairment-vs-activity-vs-participation framework.
Vignette. A 64-year-old right-handed man is admitted to inpatient rehabilitation 11 days after a left middle cerebral artery (MCA) infarct. On admission his FIM total is 56 (motor 32, cognitive 24). He has hemiplegic gait with circumduction, a stiff right knee that does not flex during swing, equinovarus foot positioning, and active right wrist extension of 12° with active right thumb extension of 11° and 10° of active extension in two additional digits. Berg Balance Scale is 38; 10-meter walk test is 0.32 m/s; MoCA is 23. After a 14-day length of stay he is discharged with a FIM total of 91. He has 8 years of formal education.
Calculate his FIM efficiency and state whether it meets the standard reimbursement benchmark; identify the dominant gait deviation and the single quadriceps muscle most appropriate for botulinum toxin injection while preserving stance-phase stability; predict his ambulation category from the 10-meter walk test threshold; classify the Berg score for fall risk; explain whether he is a CIMT candidate by Brunnstrom-stage equivalent; and adjust his MoCA for education and state whether his cognition is normal.
(Answer at the end of this chapter)
Section 1: Mirror Therapy, Functional Electrical Stimulation, and Vagus Nerve Stimulation
Bottom line: mirror therapy uses the mirror-neuron system to drive plasticity in patients with no voluntary movement (Brunnstrom 1-2) and treats post-stroke complex regional pain syndrome; functional electrical stimulation of the common peroneal nerve substitutes for cortical drive to the tibialis anterior in foot drop and requires an intact lower motor neuron; vagus nerve stimulation paired with rehabilitation improves upper-extremity recovery in chronic stroke ≥9 months out by releasing norepinephrine and acetylcholine at the moment of successful task completion.
Mirror therapy is a simple intervention that exploits the brain’s visual processing system to drive motor recovery and reduce pain after stroke. The patient sits at a table with a vertical mirror placed along the midline. The affected limb is hidden behind the mirror; the unaffected limb is positioned in front of the mirror. When the patient moves the unaffected hand, the reflection appears in the position of the affected hand, and the brain receives a visual illusion that the affected hand is moving normally. The setup hijacks the visual-motor feedback loop to drive cortical reorganization in the absence of any motor output from the affected limb.
The neurophysiological basis is the mirror neuron system, a network of neurons in premotor and parietal cortices that fires both when a person performs an action and when they observe the same action. When the patient watches the reflection of the unaffected hand moving, the mirror neuron system activates motor circuits associated with the affected hand. Functional neuroimaging during mirror therapy shows increased activation in the ipsilesional primary motor cortex (the damaged hemisphere) and premotor cortex, confirming that cortical reorganization is being driven by the visual illusion alone.
The evidence base supports mirror therapy in two settings. First, Cochrane systematic reviews show improvement in upper extremity motor function when mirror therapy is added to standard rehabilitation. Second, mirror therapy reduces pain in complex regional pain syndrome (CRPS) after stroke, where the prevailing theory is sensory-motor incongruence: the brain repeatedly sends a motor command without confirming visual or proprioceptive feedback, and the resulting error signal is interpreted as pain. Restoring visual congruence with the mirror cancels the error. Mirror therapy is inexpensive, requires no equipment beyond a mirror, has no adverse effects, and can be performed independently at home. It is appropriate even for patients with severe hemiplegia who cannot produce any voluntary movement of the affected hand, making it one of the few active recovery interventions available to patients at Brunnstrom stage 1 or 2, well below the CIMT threshold of stage 4.

Source: Wikimedia Commons, “Ramachandran-mirrorbox.svg” by Phidauex (released to public domain).
Functional electrical stimulation (FES) uses electrical current through surface or implanted electrodes to activate paralyzed or paretic muscles and produce functional movement. In stroke rehabilitation FES has two roles: a therapeutic modality during sessions to strengthen muscles and bombard the somatosensory cortex with afferent input, and an orthotic device worn throughout the day as an assistive substitute for damaged cortical drive.
The most-tested application is FES for foot drop, the single most common indication for orthotic intervention after stroke. Weakness of the ankle dorsiflexors (primarily the tibialis anterior, innervated by the deep peroneal nerve) prevents foot lift during swing phase; the foot drags and creates a tripping hazard. The traditional solution is an ankle-foot orthosis (AFO) that holds the ankle at neutral. FES offers an alternative: a surface electrode is placed over the common peroneal nerve just below the fibular head, a sensor in the shoe detects swing-phase onset, and the stimulator delivers a burst of current that fires the tibialis anterior. Stimulation timing is synchronized to the gait cycle so that dorsiflexion occurs only during swing.

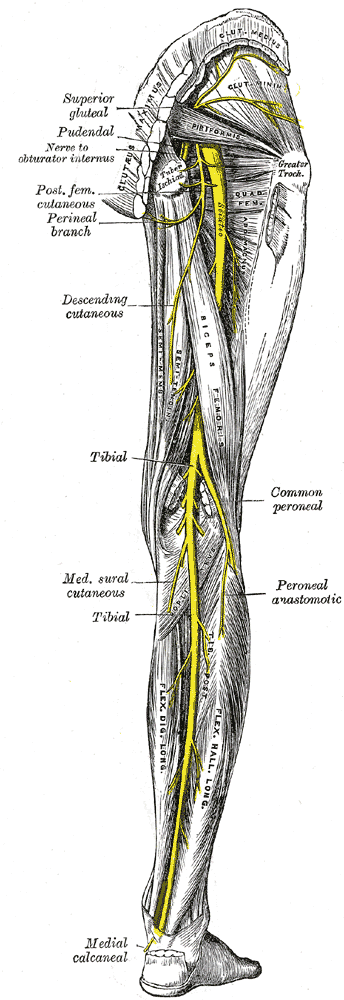
Source: Henry Gray, Anatomy of the Human Body (1918), Plate 832 via Wikimedia Commons (public domain).
FES advantages include a more physiologic gait, potential dorsiflexor strengthening, and proprioceptive feedback from active contraction (a passive AFO provides almost none). Disadvantages include cost, daily donning, skin irritation, and the requirement for an intact lower motor neuron. Stroke produces an upper motor neuron lesion, leaving the lower motor neuron intact, which is why FES works after stroke. A concurrent peroneal nerve palsy at the fibular head (for example from prolonged ICU bed rest) cuts the lower motor neuron, and FES cannot activate a denervated muscle; an AFO becomes the only viable option. Beyond foot drop, FES can target the wrist and finger extensors for grasp and release, or the shoulder muscles to reduce subluxation.
Vagus nerve stimulation (VNS) paired with rehabilitation is the newest intervention in the stroke armamentarium and represents a fundamentally different approach: rather than targeting the limb directly, VNS targets the brain’s neuromodulatory systems. VNS triggers release of norepinephrine from the locus coeruleus and acetylcholine from the basal forebrain, both of which promote synaptic plasticity and motor learning. When VNS is delivered at the precise moment the patient successfully completes a therapeutic movement, the burst of neuromodulators strengthens the neural circuits involved, amplifying Hebbian learning. Timing specificity is critical: stimulation must coincide with successful task completion.
The pivotal randomized trial published in 2021 enrolled patients with moderate-to-severe upper-extremity motor impairment at least 9 months after ischemic stroke, well into the chronic phase when spontaneous recovery has plateaued. Patients underwent surgical implantation of a vagus nerve stimulator and were randomized to active VNS plus upper-extremity rehabilitation versus sham plus the same rehabilitation. The active group gained an average of 5.8 points on the Fugl-Meyer upper extremity scale versus 2.8 points in the sham group. The Food and Drug Administration (FDA) cleared VNS paired with rehabilitation for chronic ischemic stroke patients with upper-extremity motor deficits. The conceptual significance is that VNS works at the level of the brain’s plasticity machinery itself rather than at the muscle or peripheral nerve.
High Yield — Mirror, FES, and VNS

- Mirror therapy uses the mirror neuron system in premotor and parietal cortex; activates ipsilesional primary motor cortex on fMRI; appropriate even at Brunnstrom stage 1-2 (no voluntary movement); also reduces pain in post-stroke CRPS by restoring sensory-motor congruence.
- FES for foot drop stimulates the common peroneal nerve below the fibular head to fire the tibialis anterior during swing phase. Requires an intact lower motor neuron — concurrent peroneal nerve palsy makes FES useless and forces AFO use.
- Stroke = upper motor neuron lesion; LMN intact = FES viable.
- VNS paired with rehab (FDA-cleared, 2021): chronic stroke ≥9 months post; releases norepinephrine (locus coeruleus) and acetylcholine (basal forebrain) timed to successful task completion. Active +5.8 vs sham +2.8 on Fugl-Meyer UE.
Board Trap — FES failure with concurrent peroneal palsy

A patient with stroke-related foot drop plus a peroneal nerve palsy at the fibular head from bed rest is not a candidate for FES. FES stimulates the peripheral nerve to fire the muscle; if the lower motor neuron is denervated, the muscle cannot respond. The right answer in this stem is an AFO, not FES. The discriminator is whether the lesion is purely upper motor neuron (typical post-stroke; FES works) versus mixed UMN + LMN (peroneal palsy added; only AFO works).
The brain regions that need to reorganize to support motor recovery, they light up purely through visual-motor feedback, even without any voluntary motor output from the affected limb. It’s essentially forced mental practice driven by optical input.
— CVA-07 podcast, ~04:13