Post-Stroke Dysphagia
CVA · EP 08 · STROKE
Before You Listen
Post-stroke dysphagia affects 37% to 78% of acute stroke patients depending on the screening method, and aspiration pneumonia remains the leading cause of death in the post-acute stroke period. The wide prevalence range reflects the gap between bedside screening and instrumental evaluation, which catches the silent aspirators that bedside testing always misses. This chapter maps the four phases of swallowing onto their cranial nerve substrates, contrasts the modified barium swallow study (MBSS) with the fiberoptic endoscopic evaluation of swallowing (FEES), works through the timing-of-aspiration framework that drives strategy selection, and locks in the four-week threshold for converting a nasogastric tube (NGT) to a percutaneous endoscopic gastrostomy (PEG). Memorize them cold.
- Prerequisites: baseline cranial nerve neuroanatomy (CN V, VII, IX, X, XII); upper versus lower motor neuron weakness; vascular territories of the middle cerebral artery (MCA); bedside screening versus instrumental testing.
- Runtime: 53 minutes 41 seconds.
- Topic in one line: four phases of normal swallowing and their cranial nerve mapping, MBSS as gold standard versus FEES as bedside-portable, the white-out limitation of FEES, aspiration before/during/after the swallow with paired compensatory strategies (chin tuck, head rotation, supraglottic and super-supraglottic swallows, Mendelsohn maneuver, effortful swallow), the Shaker exercise as the rehabilitative counterpart, the International Dysphagia Diet Standardisation Initiative (IDDSI) framework, the 40% silent aspiration statistic, the four-week NGT-to-PEG conversion rule, and the oral-hygiene fact that nothing-by-mouth (NPO) does not mean no oral care.
Vignette. A 68-year-old right-handed man with a left middle cerebral artery (MCA) stroke presents on hospital day 3 with right hemiparesis (face and arm worse than leg) and global aphasia. A bedside water swallow screen elicits coughing on thin liquids. A modified barium swallow study (MBSS) reveals premature bolus spillage into the pharynx with aspiration before the swallow on thin liquids, reduced laryngeal elevation with residue pooling in the pyriform sinuses after the swallow on thicker consistencies, and aspirated material with no cough response. The team must select a diet level, prescribe two compensatory strategies, decide on enteral feeding access, and counsel the family on aspiration pneumonia risk.
Which compensatory strategy targets the patient’s premature spillage, which targets the pyriform sinus residue, why is the absent cough response itself a critical finding, and what is the appropriate enteral feeding plan over the next four weeks?
(Answer at the end of this chapter)
Section 1: The Four Phases and Their Cranial Nerves
Bottom line: every dysphagia question maps a clinical finding onto one of four swallowing phases (oral preparatory, oral propulsive, pharyngeal, esophageal) and one of five cranial nerves (CN V, VII, IX, X, XII); locking the phase-to-nerve table down converts those questions into pattern recognition.
The swallow divides into four sequential phases, each with distinct anatomy, physiology, and cranial nerve control. Impairment of each phase produces a stereotyped clinical picture, and board questions reverse-engineer that picture by handing you the deficit and asking for the phase or the nerve. The first phase is the oral preparatory phase, in which food is taken in, chewed, and shaped into a cohesive bolus. The trigeminal nerve (CN V) supplies the muscles of mastication (masseter, temporalis, medial and lateral pterygoids), generating the grinding force that breaks down solids. The facial nerve (CN VII) controls the orbicularis oris (anterior lip seal) and the buccinator (the lateral cheek wall that presses food back onto the molars during chewing).
A dense lower facial droop from a left middle cerebral artery (MCA) stroke knocks out the orbicularis oris and the buccinator on the contralateral right side. The patient drools because the lip seal is broken and pockets food in the weak right cheek because the buccinator can no longer press the bolus medially onto the occlusal surface. When a vignette describes pocketing plus anterior spillage, the offending nerve is CN VII, not CN V. Practical management places food on the unaffected side, uses a mirror so the patient can monitor for pocketing, and trains the patient to sweep the weak cheek with the tongue or a finger after each bite.
The second phase is the oral propulsive (oral transit) phase. The tongue acts as a piston: the tip seals against the hard palate and a wave of posterior tongue elevation drives the bolus toward the pharynx. The hypoglossal nerve (CN XII) innervates all intrinsic and most extrinsic tongue muscles. Tongue weakness produces three hallmark findings: prolonged oral transit time (the weakened muscle cannot generate sufficient force), residual material on the hard palate after the swallow (the tongue could not strip the palate clean), and the most dangerous finding, premature spillage of bolus into the pharynx before the swallow reflex has been triggered. Premature spillage is dangerous because the laryngeal vestibule is still wide open, vocal folds are abducted, and the epiglottis has not yet inverted. Material that spills into this open pharynx falls directly toward the trachea with no protective response.
The third phase is the pharyngeal phase, the most rapid and most clinically consequential. It begins when the bolus contacts the posterior tongue base and pharyngeal wall, triggering the swallow reflex via the glossopharyngeal nerve (CN IX, sensory afferent) and the vagus nerve (CN X, motor efferent). The reflex executes in approximately 1 second. The soft palate elevates to seal the nasopharynx, the suprahyoid muscles (mylohyoid, geniohyoid, digastric, stylohyoid) yank the hyoid bone and larynx upward and forward, the epiglottis inverts to deflect the bolus laterally into the pyriform sinuses, and the upper esophageal sphincter (UES) opens to admit the bolus into the esophagus. The pharyngeal constrictors strip the bolus downward in a top-to-bottom peristaltic wave, and three layers of glottic closure (aryepiglottic folds, false vocal folds, true vocal folds) provide redundant airway protection.
The mechanics of UES opening are heavily tested. The UES is formed by the cricopharyngeus muscle, which is tonically contracted at rest to prevent reflux. Crucially, UES opening during the swallow is not an active relaxation event. It is a passive mechanical event driven by upward and forward traction on the cricoid cartilage during laryngeal elevation. The brainstem first inhibits cricopharyngeus tone, but relaxation alone does not open the door. The suprahyoid contraction yanks the cricoid (and the attached cricopharyngeus) anteriorly, mechanically pulling the sphincter open from above. If suprahyoid weakness blunts laryngeal elevation, the UES never opens fully, and bolus material backs up in the pyriform sinuses above the sphincter. Pyriform sinus residue on instrumental evaluation is the fingerprint of inadequate laryngeal elevation and incomplete UES opening.
The fourth phase is the esophageal phase, in which the bolus is carried to the stomach by peristaltic waves under vagal (CN X) parasympathetic control. The physiatrist generally does not manage esophageal dysmotility (which lives in gastroenterology), but board questions may ask the candidate to identify all four phases and their innervation.

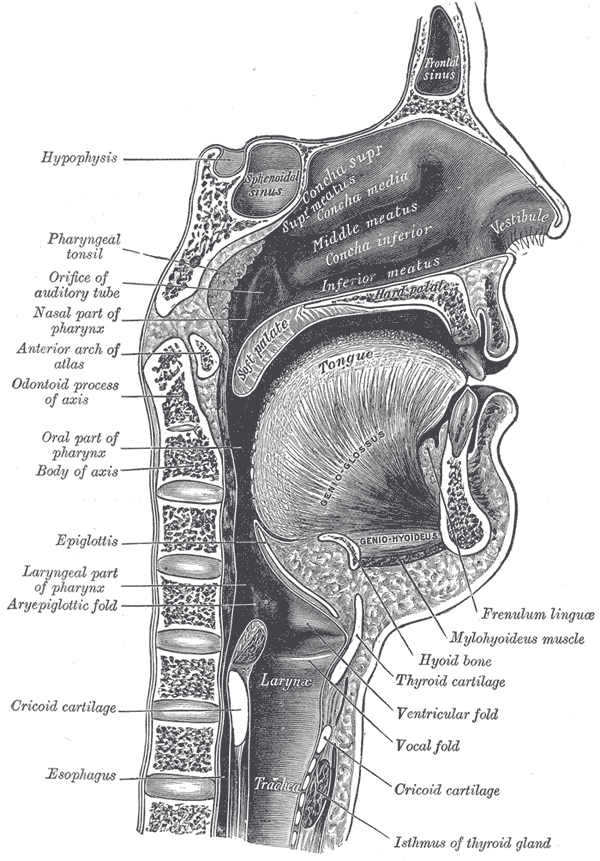
Source: Henry Vandyke Carter, “Plate 994 from Gray’s Anatomy of the Human Body” (1918), via Wikimedia Commons, Public Domain. https://commons.wikimedia.org/wiki/File:Gray994.png
High Yield — Phase-to-nerve mapping
- Pocketing + drooling = CN VII (orbicularis oris, buccinator). Place food on the unaffected side, sweep the weak cheek after each bite.
- Premature spillage + hard-palate residue + prolonged oral transit = CN XII (tongue piston). Most dangerous because the airway is still open when the bolus drops.
- Pyriform sinus residue = inadequate laryngeal elevation + incomplete UES opening. The cricopharyngeus opens passively, dragged anteriorly by the cricoid during suprahyoid contraction.
- Pharyngeal phase = CN IX (sensory) + CN X (motor). Aspiration is most likely to occur here.
- Three-layer airway closure: aryepiglottic folds, false vocal folds, true vocal folds.