Post-Stroke Aphasia, Language Disorders, and Dysarthria
CVA · EP 09 · STROKE
Before You Listen
Aphasia affects 15% to 38% of patients who suffer an ischemic stroke and is consistently ranked by patients and families as the most devastating consequence of stroke after physical paralysis. This chapter locks down the three-variable matrix (fluency, comprehension, repetition) that classifies every aphasia, walks through the four classic perisylvian aphasias with impaired repetition (Broca, Wernicke, global, conduction) and the four with preserved repetition (the three transcortical subtypes plus anomic), frames prognosis and treatment-intensity evidence, and finishes with the six dysarthrias that boards expect a candidate to match to specific lesion patterns. Memorize them cold.
- Prerequisites: vascular anatomy of the middle cerebral artery (MCA) including superior and inferior division territories; the dominant-hemisphere language model; cortical versus subcortical strokes; upper motor neuron (UMN) versus lower motor neuron (LMN) signs.
- Runtime: 1 hour 6 minutes.
- Topic in one line: the fluency-comprehension-repetition matrix, the four classic perisylvian aphasias with impaired repetition (Broca, Wernicke, global, conduction), the four with preserved repetition (anomic plus the three transcortical subtypes — motor, sensory, mixed — from watershed lesions), the dual-emboli mechanism for global aphasia without hemiparesis, the conduite d’approche fingerprint of conduction aphasia, the recovery trajectory from global to Broca to anomic, the >2-hour-per-week speech therapy threshold, constraint-induced language therapy (CILT), melodic intonation therapy (MIT), the six dysarthrias (flaccid, spastic, ataxic, hypokinetic, hyperkinetic, mixed) with their lesion patterns, and the writing test that separates aphasia from dysarthria.
Vignette. A 62-year-old right-handed man presents to the emergency department with sudden onset of difficulty speaking. He has a right facial droop and right arm weakness with leg sparing. When asked “What happened to you?” he strains for several seconds and produces “arm… no good… fell… morning.” When asked to raise his left arm, he does so immediately. When asked to repeat “no ifs, ands, or buts,” he cannot reproduce the phrase and weeps with frustration. The motor exam shows 0/5 strength in the right upper extremity and 4/5 in the right lower extremity. Computed tomography (CT) angiography is pending.
What aphasia subtype does this patient have, which middle cerebral artery (MCA) division is occluded, why does the right face and arm weakness fit the vascular anatomy, and which evidence-based language therapy is preferred for this aphasia type?
(Answer at the end of this chapter)
Section 1: The Three-Variable Matrix and the Repetition Divide
Bottom line: every aphasia is fully classified by three clinical variables (fluency, comprehension, repetition); fluency localizes anterior versus posterior; comprehension localizes the auditory processing pathway; repetition is the great divide that separates the perisylvian aphasias (impaired repetition, lesion in core network) from the transcortical aphasias (preserved repetition, lesion in watershed zone outside the core network).
The classification of every aphasia rests on three clinical variables: fluency, comprehension, and repetition. Fluency is a purely mechanical assessment of spontaneous speech output, evaluated by listening to the patient speak for 30 seconds. A fluent aphasia produces speech that flows at normal rate with normal phrase length and prosody (the musicality of speech), even if the content is meaningless. A nonfluent aphasia produces speech that is effortful, halting, and shortened to one or two words at a time, with flat telegraphic delivery and often visible facial straining. The first board shortcut: fluent aphasias localize to posterior temporal and parietal lesions; nonfluent aphasias localize to anterior frontal lesions. Anterior brain handles motor planning and execution; posterior brain handles sensory processing and meaning.
Comprehension is the brain’s ability to decode and understand spoken language. Testing it accurately is harder than it appears because patients lean on facial expressions, gesture, and environmental context. A patient may nod and smile to a routine greeting without comprehending a single word. To isolate the auditory cortex and the semantic processing centers, the examiner must hand the patient multi-step cross-modality commands stripped of social and visual cues: “Take this paper in your right hand, fold it in half, and place it on the floor.” Increasing complexity reveals the threshold where semantic understanding breaks down.
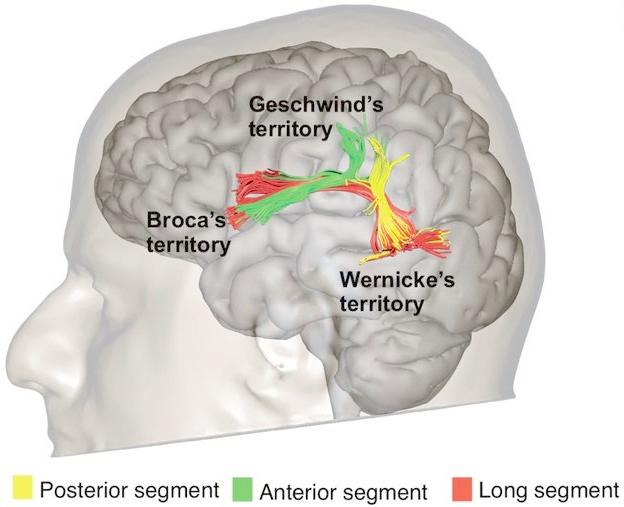
Repetition is the act of hearing a spoken phrase and reproducing it verbatim, and it is the linchpin of aphasia classification. Repetition requires the integrity of the dominant-hemisphere perisylvian network: Wernicke area in the posterior superior temporal gyrus (where sounds become meaning), Broca area in the inferior frontal gyrus (where concepts become motor programs), and the arcuate fasciculus (the white matter cable arching from Wernicke through the parietal lobe to Broca). The classic test phrase is “no ifs, ands, or buts.” Repetition is a closed-loop task that demands the acoustic signal travel intact from Wernicke through the arcuate fasciculus to Broca. If any segment of the loop is broken, repetition fails.
The single most important dividing line in the classification system is repetition. The classic perisylvian aphasias with impaired repetition are Broca, Wernicke, global, and conduction — each damages a component of the core perisylvian network. Transcortical aphasias spare the perisylvian network entirely and preserve repetition because the damage lies outside the core network in the watershed zones between major vascular territories. Anomic aphasia is the special case: anatomically perisylvian (left angular gyrus / temporoparietal junction) but with preserved repetition, since neither the arcuate fasciculus nor Broca/Wernicke proper is interrupted. When a board question presents any aphasia with preserved repetition plus impaired comprehension or fluency, immediately select a transcortical subtype; if repetition is preserved with intact comprehension and fluency but a prominent word-finding deficit, the answer is anomic.

Source: Wikimedia Commons (PD/CC-BY licensed; verify at file page).
High Yield — The repetition divide

- Three classification variables: fluency (anterior vs posterior), comprehension (intact vs impaired), repetition (intact, impaired, or preserved).
- Perisylvian aphasias with impaired repetition = Broca, Wernicke, global, conduction (damage the core network). Anomic aphasia is anatomically perisylvian (angular gyrus) but preserves repetition.
- Transcortical aphasias (motor, sensory, mixed) lie outside the core network in watershed zones and preserve repetition.
- Repetition tests the arcuate fasciculus loop: Wernicke area to Broca area through the arcuate fasciculus.
- Test phrase: “no ifs, ands, or buts.”
- Comprehension testing must strip away gesture and context: use multi-step cross-modality commands, not yes/no greetings.