MEDREH · EP 04 · BURNS
Before You Listen
Episode Setup
- Topic in one line: burn depth classification with the painless full-thickness pearl, total body surface area (TBSA) by Rule of Nines vs Lund-Browder (most accurate, age-adjusted, peds in PEDS-11), Parkland formula (4 mL × kg × percent TBSA, half in first 8 hours from time of burn), Jackson three-zone model with stasis as the salvageable zone, topical antimicrobials with distinguishing side effects (silver sulfadiazine causes leukopenia, mafenide acetate is a carbonic anhydrase inhibitor causing metabolic acidosis but penetrates eschar, silver nitrate causes hyponatremia/hypochloremia, bacitracin for face), anti-deformity positioning for every major joint, pressure garments at 25 mmHg for 23-24 hours per day for 12-18 months, inhalation injury (supraglottic thermal, subglottic chemical) with carbon monoxide poisoning where pulse oximetry is unreliable, electrical burn complications (arrhythmias, compartment syndrome, rhabdomyolysis, delayed cataracts), heterotopic ossification (HO) at the elbow in burns vs the hip in TBI/SCI, split- vs full-thickness skin grafts, and American Burn Association (ABA) transfer criteria.
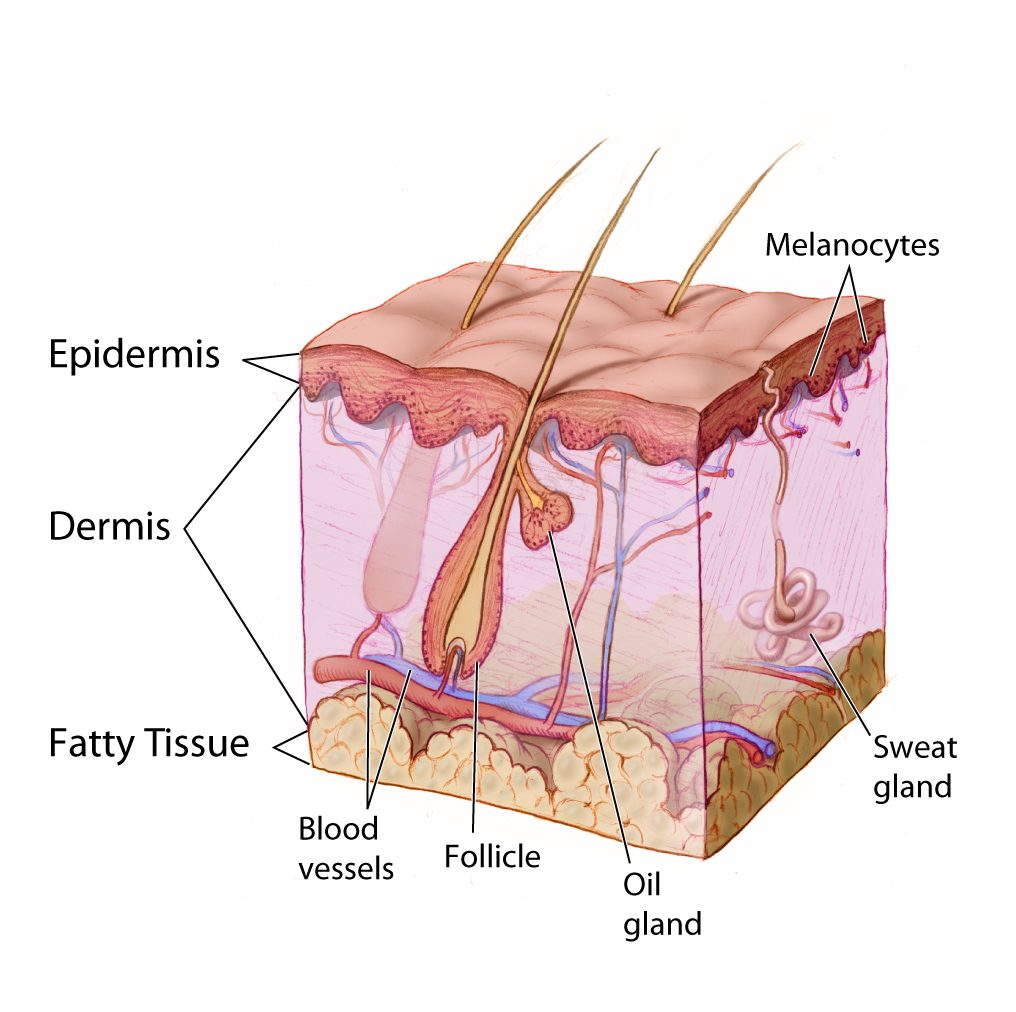
- Prerequisites: skin layers (epidermis, papillary dermis, reticular dermis, subcutaneous tissue), basic metabolic acidosis from carbonic anhydrase inhibition, the carboxyhemoglobin spectrum and pulse oximeter limitations, and the principle that scar tissue contracts in the direction opposite of anatomic function.
- Runtime: 1 hour 6 minutes.
Vignette. A 35-year-old man weighing 70 kg presents to the emergency department 90 minutes after a house fire with deep partial-thickness and full-thickness burns covering both arms (anterior and posterior), the anterior trunk, and the anterior aspects of both thighs. He has singed nasal hairs, carbonaceous sputum, and a hoarse voice. Pulse oximetry reads 98 percent on room air. Co-oximetry shows a carboxyhemoglobin level of 32 percent. He is alert. Burn depth is full-thickness on the dorsa of both hands. The remainder of the burns are deep partial-thickness.
What is his estimated TBSA by the Rule of Nines, what is his Parkland formula fluid resuscitation in the first 24 hours and how is it timed, what does the pulse oximetry reading actually mean and what is the next intervention, what is the anti-deformity position for his hands, and where does he most commonly develop heterotopic ossification compared to a traumatic brain injury patient?
(Answer at the end of this chapter)
Section 1: Burn Depth, Total Body Surface Area, and the Parkland Formula
Bottom line: burn depth is superficial (epidermis only, painful, NOT in TBSA), superficial partial-thickness (blisters, very painful, heals 7-21 days), deep partial-thickness (decreased sensation, heals 3-9 weeks, often grafted), full-thickness (painless, leathery, requires grafting), and subdermal (fat, muscle, tendon, or bone). Painless = full-thickness because all sensory endings are destroyed. Adult Rule of Nines: head 9, each upper extremity 9, anterior trunk 18, posterior trunk 18, each lower extremity 18, perineum 1. The Lund-Browder chart is the most accurate (age-adjusted, preferred in peds, covered in PEDS-11). The palmar surface method uses the patient’s palm with fingers as ~1 percent of TBSA. Parkland (Baxter) formula: 4 mL × kg × percent TBSA of lactated Ringer in 24 hours, half in the first 8 hours from time of burn (not presentation), half over the next 16 hours. Adequacy judged by urine output: 0.5-1 mL/kg/hr adults, 1 mL/kg/hr children.
Burn depth determines prognosis, healing time, and the need for surgery.
A superficial burn (first-degree, e.g., sunburn) involves only the epidermis. Skin is red, dry, painful, and blanches. No blisters. Healing in 3-7 days without scarring. Superficial burns are NOT counted in the TBSA calculation for fluid resuscitation.
A superficial partial-thickness burn (superficial second-degree) extends into the superficial papillary dermis. Hallmark: blisters (bullae). Wound base is pink, moist, and very painful because sensory endings are exposed and intact. Heals in 7-21 days by re-epithelialization from surviving skin appendages.
A deep partial-thickness burn extends into the reticular dermis. Sensation is decreased. Wound is mottled pink and white, less moist, and may not blanch. Heals in 3-9 weeks; frequently requires skin grafting.
A full-thickness burn (third-degree) destroys the entire epidermis and dermis. The wound is painless because all sensory endings have been destroyed. Painless = full-thickness is the critical pearl. Appearance: white, waxy, brown, or leathery with dry firm eschar. Cannot heal by re-epithelialization; requires excision and skin grafting.
A subdermal burn (fourth-degree) extends into fat, muscle, tendon, or bone, typically from prolonged exposure, electrical injury, or high-temperature contact. Requires extensive surgical management and may require amputation.

Source: Don Bliss / National Cancer Institute, Wikimedia Commons, Public Domain
Total body surface area (TBSA) estimation guides fluid resuscitation, transfer criteria, and prognosis. Only partial-thickness and full-thickness burns are counted.
The Rule of Nines in adults: head and neck 9 percent, each upper extremity 9 percent, anterior trunk 18 percent, posterior trunk 18 percent, each lower extremity 18 percent, perineum 1 percent. Total 100 percent.
In pediatric patients proportions differ because children have larger heads and smaller lower extremities (infant head 18 percent, each lower extremity 14 percent). The Lund-Browder chart is the most accurate (age-adjusted). Detailed pediatric burn rehabilitation is covered in PEDS-11.
The palmar surface method uses the patient’s palm with fingers as ~1 percent of TBSA, useful for small or scattered burns.

Source: Jmarchn, Wikimedia Commons, CC BY-SA 3.0
The Parkland (Baxter) formula calculates first-24-hour fluid resuscitation: 4 mL × body weight (kg) × percent TBSA of lactated Ringer. The first half is delivered in the first 8 hours from time of burn (not from presentation). The second half over the next 16 hours.
Worked example: 70 kg patient with 40 percent TBSA: 4 × 70 × 40 = 11,200 mL (11.2 L) of LR in 24 hours. First 5,600 mL in the first 8 hours from time of burn; remaining 5,600 mL over the next 16 hours.
Target urine output: 0.5-1 mL/kg/hr in adults, 1 mL/kg/hr in children.
High Yield — Depth, TBSA, Parkland
- Burn depth: superficial (epidermis only, painful, NOT in TBSA) → superficial partial (blisters, very painful, heals 7-21 d) → deep partial (decreased sensation, heals 3-9 wk, may graft) → full-thickness (painless, leathery, requires grafting) → subdermal (fat, muscle, bone).
- Painless burn = full-thickness (single sharpest pearl).
- Rule of Nines (adult): head 9, each UE 9, anterior trunk 18, posterior trunk 18, each LE 18, perineum 1.
- Lund-Browder = most accurate (age-adjusted), preferred in peds.
- Palmar surface = ~1 percent of TBSA.
- Parkland: 4 × kg × percent TBSA mL LR in 24 h; half in first 8 h from time of burn, half over next 16 h.
- Target urine output: 0.5-1 mL/kg/hr adult, 1 mL/kg/hr child.
Mnemonic — “Nine head, nine arm, eighteen torso side, eighteen leg, one perineum”
The adult body sums to 100. Head 9. Each arm 9. Each torso side 18 (anterior, posterior). Each leg 18. Perineum 1. Memorize the count, then practice on a few cases. The pediatric chart shifts mass toward the head and away from the legs because the child has a relatively larger cranium.
If they present with a wound that looks white, waxy, brown, or kind of leathery, with absolutely zero capillary refill and zero blanching when you press on it, and they tell you it does not hurt at all, you are looking at a full thickness third degree burn.
— MEDREH-04 podcast, ~00:21