MEDREH · EP 10 · LYMPHEDEMA
Before You Listen
Episode Setup
- Topic in one line: lymphedema as the chronic accumulation of protein-rich interstitial fluid from impaired lymphatic transport, classified as primary (Milroy congenital, praecox/Meige around puberty, tarda after age 35) versus secondary (post-axillary lymph node dissection (ALND) breast cancer in the United States, lymphatic filariasis worldwide, recurrent cellulitis, surgery, trauma, malignant obstruction); the International Society of Lymphology (ISL) staging system from Stage 0 (latent, transport impaired without visible edema) through Stage 3 (lymphostatic elephantiasis with papillomatosis and hyperkeratosis); the pathognomonic Stemmer sign (inability to pinch a skin fold at the base of the second toe or finger); lymphoscintigraphy as the gold-standard imaging study; complete decongestive therapy (CDT) as the gold-standard treatment in a Phase 1 intensive reductive phase (manual lymphatic drainage (MLD), multilayer short-stretch bandaging, exercise, skin care over 2-6 weeks) followed by a Phase 2 lifelong maintenance phase (custom 30-40 millimeter of mercury (mmHg) compression garment, self-MLD, exercise, skin care); the ankle-brachial index (ABI) thresholds (>0.8 full compression, 0.5-0.8 modified, <0.5 absolute contraindication) that gate compression safety; and the three-way differential of lymphedema versus chronic venous insufficiency (CVI) edema versus lipedema.
- Prerequisites: lymphatic anatomy (superficial cutaneous network, deep system traveling along veins, thoracic duct), basic principles of compression therapy, and the cellulitis differential.
- Runtime: 1 hour 4 minutes.
Vignette. A 58-year-old woman is admitted to your inpatient rehabilitation facility (IRF) for deconditioning 6 weeks after right modified radical mastectomy with axillary lymph node dissection (12 nodes removed, 3 positive) and adjuvant axillary radiation for stage two-B breast cancer. She has noticed progressive heaviness and a tight feeling in her right arm over the past 10 days. Her right arm is visibly larger than her left, with a 4 cm circumferential difference at the mid-forearm and 5 cm at the mid-upper arm. The dorsum of her right hand is swollen, and you cannot pinch a skin fold at the base of her right second finger. The skin is intact but slightly tight. Her right elbow flexion is mildly limited by the swelling. She wonders aloud whether she should have started compression “before this got bad” and asks whether she can still travel to her son’s wedding by air in three weeks.
Which form of secondary lymphedema is this, what stage on the ISL classification, what bedside finding distinguishes it from chronic venous insufficiency, what is the gold-standard treatment program in its two phases, and what specific air-travel guidance and prospective surveillance message should you give her?
(Answer at the end of this chapter)
Section 1: Lymphatic Anatomy, Primary Versus Secondary Lymphedema, and Why the Fluid Is Protein-Rich
Bottom line: lymphedema is the chronic accumulation of protein-rich interstitial fluid from impaired lymphatic transport, and the protein-rich nature drives fibrosis, adipose deposition, chronic inflammation, and infection susceptibility, and distinguishes lymphedema mechanistically from venous edema; the lymphatic system has three compartments (superficial cutaneous network, deep system along veins, central thoracic duct emptying into the left subclavian vein); primary lymphedema is age-stratified into Milroy (birth to 2 years, autosomal dominant FLT4/VEGFR-3, ~10 percent), praecox/Meige (2 to 35 years, often puberty, 65-80 percent, female 10:1), and tarda (after 35, ~10 percent); secondary lymphedema is far more common and dominated in the US by post-cancer treatment (BCRL after ALND 20-40 percent, after SLNB 5-8 percent) and worldwide by lymphatic filariasis (Wuchereria bancrofti, ~120 million people).
Lymphedema is the chronic accumulation of protein-rich interstitial fluid caused by impaired lymphatic transport. The protein-rich nature drives progression: trapped proteins osmotically draw fluid in, fibroblasts proliferate, collagen deposits, adipose hypertrophies, and bacteria thrive in the stagnant proteinaceous medium. Diuresis removes water but concentrates residual proteins and accelerates fibrosis, which is why diuretics do not work. Every treatment principle (compression for hydrostatic clearance, MLD for redirection through patent territories, skin care to interrupt the cellulitis-fibrosis cycle) follows from this anchor.
The lymphatic system has three functional compartments. The superficial system is a dense cutaneous network organized into watershed territories (sagittal midline, umbilical-level axillary watershed). When a regional outflow is obstructed, competent manual lymphatic drainage (MLD) redirects superficial flow across these watersheds into adjacent functioning territories. The deep system travels alongside the major veins and drains muscle and viscera, propelled by intrinsic lymphatic smooth muscle and the skeletal muscle pump. The thoracic duct carries lymph from the entire body below the diaphragm and the left side above the diaphragm into the left subclavian vein. The right head/neck/upper chest drains via the right lymphatic duct into the right subclavian vein.
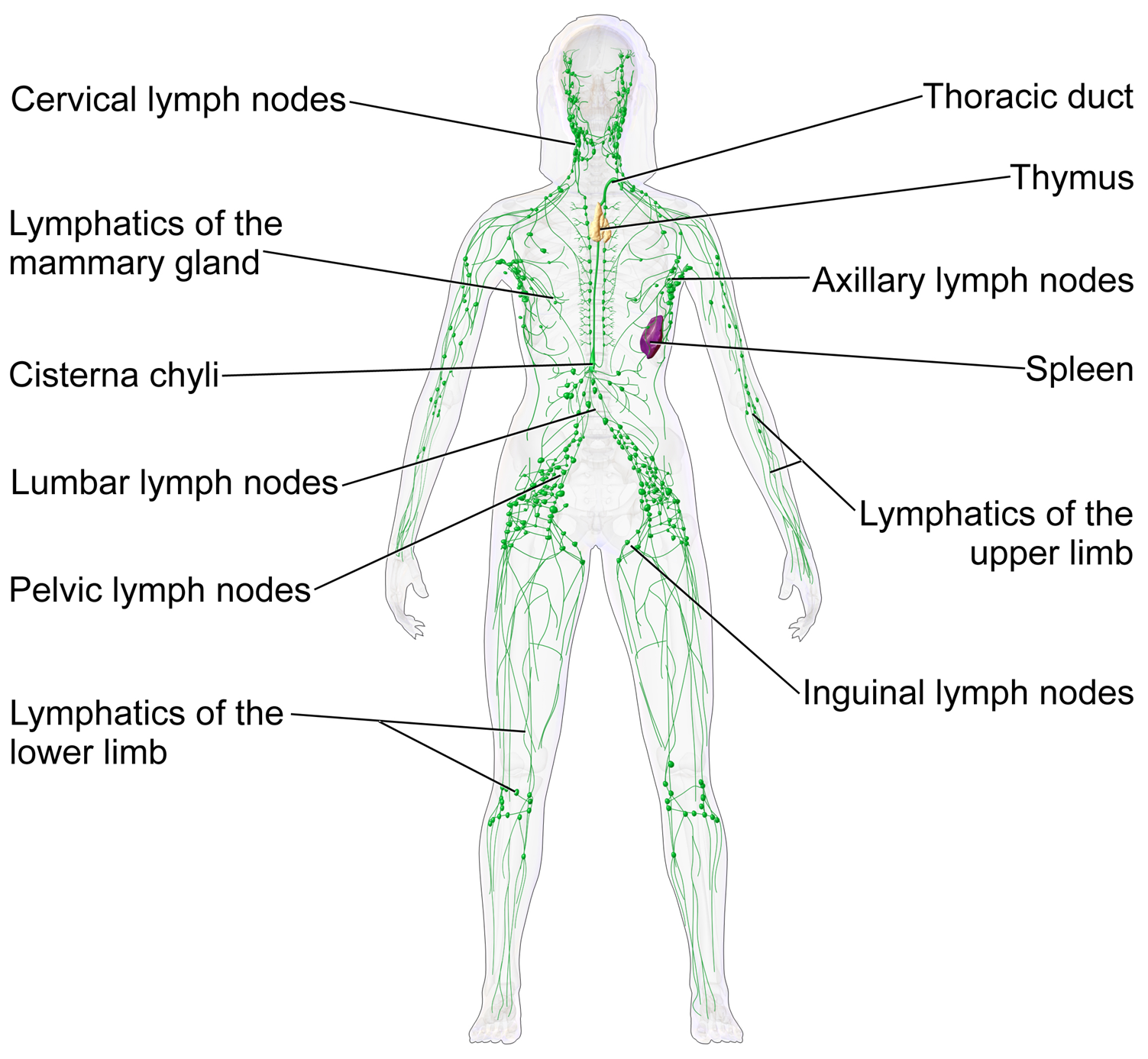
Source: BruceBlaus / Blausen Medical, Wikimedia Commons, CC BY 3.0
Primary lymphedema is congenital developmental abnormality (aplasia, hypoplasia, hyperplasia) and is subclassified by age of onset. Milroy disease presents birth to age 2, is autosomal dominant from mutations in FLT4 encoding vascular endothelial growth factor receptor 3 (VEGFR-3), typically bilateral lower extremity, ~10 percent of primary cases. Praecox (Meige disease) presents age 2 to 35, most commonly at puberty, is the most common primary form (65-80 percent), with a 10:1 female predominance, usually unilateral. Tarda presents after age 35, ~10 percent, often triggered by minor insult on preexisting subclinical insufficiency.
Secondary lymphedema is far more common. In the US, the most common cause is cancer treatment with regional lymph node dissection and/or radiation, with breast-cancer-related lymphedema (BCRL) following axillary lymph node dissection (ALND) as the prototype. BCRL develops in 20-40 percent after ALND and 5-8 percent after sentinel lymph node biopsy (SLNB) alone. Pelvic and inguinal node dissection causes lower extremity lymphedema by the same mechanism. Worldwide, the most common cause is lymphatic filariasis (Wuchereria bancrofti, mosquito-transmitted), affecting more than 120 million people. Other secondary causes include surgery and trauma, recurrent cellulitis (each episode further damages vessels), severe obesity (BMI > 40), and malignant obstruction.
High Yield — Anatomy and classification

- Lymphedema = chronic accumulation of protein-rich interstitial fluid from impaired lymphatic transport. Protein-rich nature drives fibrosis, adipose hypertrophy, infection. Diuretics do not work and accelerate fibrosis.
- Three lymphatic compartments: superficial (cutaneous, with watershed territories MLD redirects across), deep (alongside veins, muscle pump), thoracic duct (empties into the left subclavian vein).
- Primary: Milroy (birth-2 yr, autosomal dominant, FLT4/VEGFR-3, ~10%); Praecox/Meige (2-35 yr, most common at puberty, 65-80%, female 10:1); Tarda (>35 yr, ~10%).
- Secondary: US #1 = breast-cancer-related lymphedema after ALND (20-40% post-ALND, 5-8% post-SLNB); worldwide #1 = lymphatic filariasis (Wuchereria bancrofti), ~120 million infected.
- Other secondary: surgery, trauma, recurrent cellulitis, obesity (BMI > 40), malignant obstruction, phlebolymphedema.
Mnemonic — “Protein draws fluid; fluid draws fibrosis; fibrosis draws bacteria”

The chain reaction of untreated lymphedema runs in three steps. Trapped proteins osmotically draw additional fluid into the interstitium. The chronically distended interstitium recruits fibroblasts and adipose hypertrophy. The proteinaceous medium and the broken skin barrier invite cellulitis, and each cellulitis episode kills more lymphatics, tightening the loop. Every component of complete decongestive therapy interrupts one of these three steps.