MSK · EP 04 · ELBOW
Before You Listen
Episode Setup
- Topic in one line: the elbow as three articulations inside one shared synovial capsule, the anterior band of the ulnar collateral ligament (UCL) as the primary valgus stabilizer, the medial-versus-lateral epicondyle dichotomy that drives epicondylitis pattern recognition, and the five phases of throwing biomechanics that explain why every overhead athlete hurts the medial elbow first and the posterior compartment second.
- Prerequisites: brachial plexus organization (lateral, posterior, and medial cords), nerve-by-nerve elbow flexor and extensor innervation, and the principle that overuse tendinopathy is angiofibroblastic degeneration rather than acute inflammation.
- Runtime: 1 hour 5 minutes.
Vignette. A 28-year-old right-hand-dominant minor-league pitcher presents with a 6-week history of medial elbow pain that intensifies in the late cocking phase of his pitching motion. He denies acute injury but reports a 4 mph drop in fastball velocity and intermittent paresthesias along the small finger after long bullpen sessions. On examination he has point tenderness 1 cm distal to the medial epicondyle, a positive valgus stress test at 25 degrees of elbow flexion with a soft endpoint and 3 mm of medial joint opening compared to the contralateral side, and a positive Tinel sign at the cubital tunnel. The static valgus extension overload maneuver is painless throughout the arc, but the dynamic valgus extension test reproduces sharp pain at the last 7 degrees of terminal extension.
Which structure is the primary anatomical lesion driving the medial pain, what does the dynamic-but-not-static finding indicate about the posterior compartment, why does the small-finger paresthesia sit comfortably on top of the same diagnosis, and what is the surgical reconstruction of choice in a high-demand thrower whose conservative course fails?
(Answer at the end of this chapter)
Section 1: The Three-Joint Capsule, Range of Motion, and the Carrying Angle
Bottom line: the elbow is a complex of three articulations (the humeroulnar hinge, the humeroradial joint, and the proximal radioulnar pivot) all enclosed in one synovial capsule, which is why a minor radial head fracture floods the entire joint and locks down flexion, extension, and rotation simultaneously; normal range of motion is 135 degrees of flexion, 0 to 5 degrees of extension, and 90/90 supination and pronation; the carrying angle is approximately 5 degrees of valgus in males and 10 to 15 degrees in females, and any value greater than 20 degrees is cubitus valgus and predisposes the patient to ulnar neuropathy through cumulative traction on the nerve as it courses behind the medial epicondyle.
The elbow is not a simple hinge. It comprises three distinct articulations enclosed inside one synovial capsule. The humeroulnar joint is the true hinge, formed by the trochlea of the distal humerus articulating with the trochlear notch of the proximal ulna. It drives flexion and extension and locks the olecranon into the olecranon fossa at full extension, providing substantial bony stability when the elbow is straight. The humeroradial joint sits on the lateral side, formed by the capitellum articulating with the concave proximal surface of the radial head; it participates in both flexion-extension and forearm rotation. The proximal radioulnar joint is the pivot, formed between the radial head and the radial notch of the ulna and held in place by the annular ligament; rotation of the radius around the ulna drives forearm pronation and supination, working in tandem with the distal radioulnar joint at the wrist.
The single-capsule concept anchors the clinical reasoning. Because all three joints share one synovial cavity, any pathology that produces effusion (fracture, hemarthrosis, septic arthritis, inflammatory synovitis) affects every articulation simultaneously. A hemarthrosis from a non-displaced radial head fracture does not merely limit forearm rotation; it distends the entire capsule, restricting flexion, extension, and rotation in a single global pattern. Three joints, one capsule: hold this image and the clinical picture organizes itself.
Normal elbow range of motion is tested as discrete numbers. Flexion runs to 135 degrees, and most activities of daily living can be performed with approximately 130 degrees. Extension is 0 to 5 degrees; up to 5 degrees of hyperextension falls within the normal range, particularly in females and individuals with generalized ligamentous laxity. Supination is 90 degrees and pronation is 90 degrees, producing a 180-degree rotational arc that requires both the proximal and distal radioulnar joints to be intact. Commit to memory: 135 / 0-5 / 90 / 90.
The carrying angle is one of the most heavily tested alignment concepts. With the arms extended and forearms supinated, the forearm angles laterally away from the trunk to allow the arms to clear the hips during gait. The normal carrying angle is approximately 5 degrees of valgus in males and 10 to 15 degrees of valgus in females. The threshold for abnormality is greater than 20 degrees, classified as cubitus valgus. A chronically increased valgus angle places the ulnar nerve under increased traction behind the medial epicondyle, and a stem that pairs cubitus valgus with paresthesias in the small finger and ulnar half of the ring finger is asking about an ulnar neuropathy from cumulative stretch injury.
The collateral ligaments stabilize the elbow against angular forces. The ulnar collateral ligament, also termed the medial collateral ligament, has three components: anterior band, posterior band, and transverse ligament. The anterior band of the UCL is the primary restraint against valgus stress throughout the functional flexion arc and is the structure reconstructed during Tommy John surgery. The lateral collateral ligament complex stabilizes the lateral side; the lateral ulnar collateral ligament is its key stabilizer and the structure most commonly disrupted in posterolateral rotatory instability. The annular ligament wraps around the radial head; in young children, a sudden longitudinal pull on an extended forearm can slip the annular ligament over the radial head, producing nursemaid’s elbow.
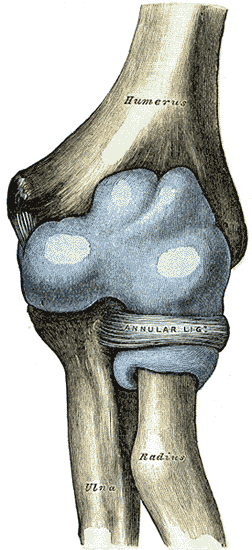
Source: Henry Vandyke Carter, Gray’s Anatomy (Plate 331), Wikimedia Commons, Public Domain. Anterior view of the distended elbow joint capsule enveloping the humeroulnar, humeroradial, and proximal radioulnar articulations.
High Yield — Capsule, motion, and carrying angle

- Three joints / one capsule: humeroulnar (hinge) + humeroradial + proximal radioulnar; effusion from any cause floods all three and limits global motion.
- Range of motion: flexion 135 / extension 0-5 / supination 90 / pronation 90.
- Carrying angle: 5 degrees male, 10-15 degrees female; greater than 20 degrees = cubitus valgus → ulnar neuropathy from chronic traction.
- Anterior band of the UCL = primary valgus stabilizer (Tommy John target).
- Lateral ulnar collateral ligament = primary lateral stabilizer (posterolateral rotatory instability).
- Annular ligament = radial head seat belt; slips over the head in nursemaid’s elbow.
Mnemonic — “Three joints, one capsule”
When a stem describes globally restricted elbow motion after a small intra-articular injury, the answer hinges on the single shared capsule. Hemarthrosis cannot stay local. Treat radial head fractures with early range of motion within 3 to 5 days; prolonged immobilization produces flexion contractures faster at the elbow than at almost any other joint.
Three joints, one capsule. A tiny crack on one bone paralyzes all three joints, which makes so much sense of what we see in the clinic. Patients come in with a localized injury, but their whole arm is just frozen.
— MSK-04 podcast, ~2:26