MSK · EP 09 · MUSCULOSKELETAL
Before You Listen
Episode Setup
- Topic in one line: the geriatric hip fracture and its decision tree, intracapsular versus extracapsular anatomy and how that maps to avascular necrosis (AVN) risk via the medial femoral circumflex artery, the Garden classification of femoral neck fractures, total hip arthroplasty (THA) precaution sets by surgical approach, and the four pediatric hip diagnoses that physiatrists must never miss (Legg-Calve-Perthes, slipped capital femoral epiphysis, developmental dysplasia of the hip, and transient synovitis).
- Prerequisites: MSK-08 hip anatomy (the medial femoral circumflex artery as the dominant adult femoral head blood supply), basic understanding of the obturator nerve referral pattern from hip to knee, the concept of physeal weakness in adolescence, and the rehabilitation principle that posterior surgical exposures violate posterior structures and create posterior-direction instability.
- Runtime: approximately 1 hour 18 minutes.
Vignette. A 13-year-old boy with a body mass index in the 95th percentile presents to the clinic with three weeks of progressive medial knee pain on the right side. He has no history of acute knee trauma. On examination the right knee has a full and painless range of motion with no joint line tenderness, no effusion, and a normal Lachman test. When the examiner passively flexes the right hip, the leg involuntarily swings into external rotation, and internal rotation of the hip is markedly restricted. Anteroposterior and frog-leg lateral radiographs of the pelvis are obtained.
Which hip diagnosis explains the knee pain, what is the obligate physical-examination finding the examiner just elicited, what radiographic line is used to confirm the diagnosis, and what is the correct urgent management even if the slip appears to be mild on the radiograph?
(Answer at the end of this chapter)
Section 1: The Geriatric Hip Fracture and the Garden Classification
Bottom line: hip fractures in the elderly carry a one-year mortality of 20 to 30 percent, and management hinges on whether the fracture line crosses the joint capsule; intracapsular femoral neck fractures threaten the medial femoral circumflex artery and are graded by the Garden classification (I-II nondisplaced and pinned with cannulated screws, III-IV displaced and replaced with arthroplasty), while extracapsular intertrochanteric fractures preserve femoral head blood supply but bleed substantially and are fixed with a sliding hip screw or an intramedullary nail.
Hip fractures are among the most consequential diagnoses in rehabilitation medicine. The one-year mortality after a geriatric hip fracture is between 20 and 30 percent, meaning roughly one in four elderly patients who fracture a hip will not survive the following year. The mortality is rarely from the fracture itself but from the cascade of complications it precipitates: venous thromboembolism, pneumonia, deconditioning, delirium, and the loss of physiologic reserve. Among survivors, only about half ever return to their pre-injury level of function. For the physiatrist managing these patients, the diagnosis demands the same urgency as a malignancy. Early mobilization, deep vein thrombosis (DVT) prophylaxis, nutritional optimization, and vigilant complication surveillance stand between the patient and the mortality statistic.
The classification and management of hip fractures hinge entirely on the anatomic location of the fracture line relative to the hip joint capsule. The two major categories are intracapsular fractures, meaning femoral neck fractures, and extracapsular fractures, meaning intertrochanteric and subtrochanteric fractures. The distinction is not academic. It determines whether the blood supply to the femoral head is at risk, which in turn determines whether the surgeon pins the bone or replaces it.

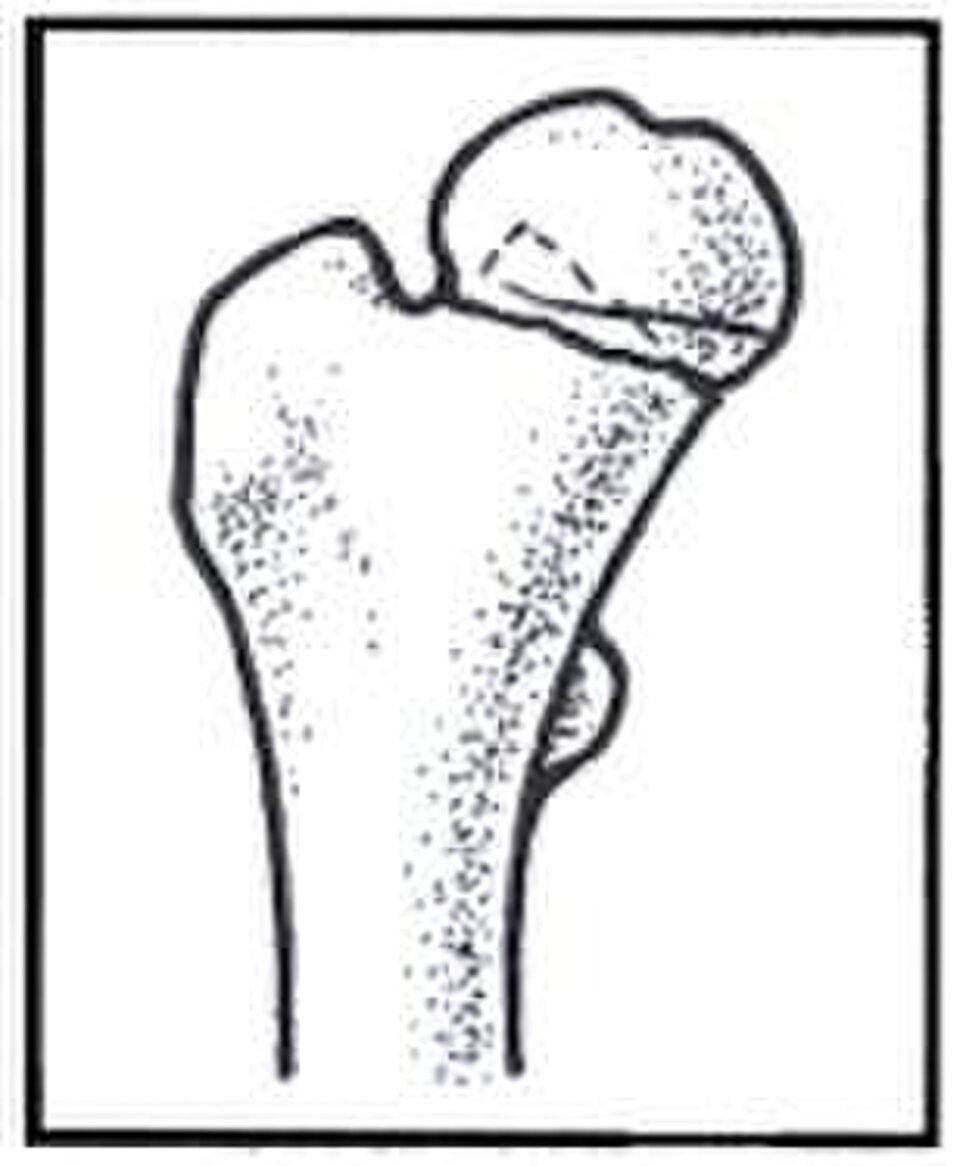
Source: Orthopaedic Trauma Association (1999), Wikimedia Commons, CC BY 2.5.
Femoral neck fractures are intracapsular. The fracture line runs through the femoral neck inside the joint capsule. The femoral head receives its arterial supply primarily from the retinacular branches of the medial femoral circumflex artery, which travel along the femoral neck inside the capsule. When the neck fractures, those vessels can be torn or kinked. If blood flow is interrupted, the femoral head undergoes avascular necrosis, the bone dies, and the fracture fails to heal as nonunion. The risk of AVN is directly proportional to the degree of fracture displacement, which is the central principle that drives the Garden classification.
The Garden classification stages femoral neck fractures by displacement on the anteroposterior (AP) radiograph. Garden I is an incomplete or impacted fracture in which the fracture line is visible but the femoral head is impacted into a slight valgus position with the trabeculae still in partial continuity. This is the most stable pattern. Garden II is a complete but nondisplaced fracture in which the fracture extends through the femoral neck but the fragments have not shifted. Both Garden I and Garden II fractures are nondisplaced, the retinacular vessels are likely intact, and the AVN rate is on the order of 10 to 15 percent. Treatment is internal fixation with percutaneous cannulated screws.
Garden III is a partially displaced fracture in which the fragments have shifted but maintain some bony contact. The retinacular vessels are stretched and may be partially disrupted. Garden IV is a completely displaced fracture in which the femoral head is entirely separated from the femoral neck and the retinacular vessels are almost certainly torn. Garden III and Garden IV are displaced fractures, and the AVN rate climbs to 30 to 40 percent. The risk of nonunion is also substantial. Pinning a head whose blood supply has been destroyed is futile because the dead head will collapse, so displaced femoral neck fractures in elderly patients are treated with arthroplasty rather than internal fixation. In younger patients with displaced femoral neck fractures, urgent anatomic reduction and internal fixation is attempted to try to restore blood flow and salvage the native head, but the AVN risk remains high.
Within the arthroplasty category, a hemiarthroplasty replaces only the femoral side, leaving the patient’s native acetabulum intact. A total hip arthroplasty (THA) replaces both the femoral head and the acetabular socket. In elderly patients with low functional demands and a normal native acetabulum, hemiarthroplasty is common. A bipolar hemiarthroplasty uses a dual-bearing design in which a small metal ball articulates within a larger polyethylene shell, distributing wear across two surfaces. In active elderly patients or those with pre-existing acetabular arthritis, total hip arthroplasty provides better long-term outcomes.
Intertrochanteric fractures occur between the greater and lesser trochanters and are the hallmark injury of the elderly osteoporotic patient. Because the fracture is extracapsular, the retinacular vessels are proximal to the fracture and remain intact, AVN risk is low, and the femoral head is preserved. The bone in the intertrochanteric region is predominantly cancellous and highly vascular, so these fractures bleed profusely and patients can lose several grams of hemoglobin into the thigh. Treatment is always surgical fixation rather than replacement, with the standard options being a sliding hip screw (also called a dynamic hip screw) or an intramedullary nail. Both devices stabilize the fracture and allow controlled compression at the fracture site as the patient bears weight; the intramedullary nail is favored for unstable patterns because its central position neutralizes bending forces more effectively than a laterally placed plate.
Femoral neck stress fractures sit one notch up the urgency ladder because they can cross from a stress reaction into a complete displaced femoral neck fracture under continued load. The femoral neck experiences two types of mechanical stress during weight bearing: the superior cortex is under tension and the inferior cortex is under compression. A tension-side (superior cortex) stress fracture is a surgical emergency because tensile forces are pulling the bone apart, and a tension-side fracture has a high risk of completing and displacing into a true femoral neck fracture, which would then disrupt the medial femoral circumflex artery and produce AVN. A compression-side (inferior cortex) stress fracture is being pushed together by weight-bearing forces, is inherently more stable, and may be treated conservatively with protected weight bearing if nondisplaced. The board-critical pairing is: tension = superior = surgical emergency; compression = inferior = may treat conservatively.
High Yield — Femoral neck fractures and the Garden classification
- Intracapsular = femoral neck; threatens medial femoral circumflex artery; AVN risk proportional to displacement.
- Garden I-II = nondisplaced; AVN ~10-15 percent; treat with percutaneous cannulated screws.
- Garden III-IV = displaced; AVN ~30-40 percent; treat with arthroplasty (hemi or total) in elderly; urgent anatomic reduction + fixation in young patients.
- Intertrochanteric = extracapsular; low AVN risk; substantial blood loss; treat with sliding hip screw or intramedullary nail.
- Femoral neck stress fracture: tension-side (superior) = surgical emergency; compression-side (inferior) = may treat conservatively.
Board Trap — “Pin the displaced femoral neck fracture and hope for the best”
A vignette describes a 78-year-old who falls from standing and has a Garden IV displaced femoral neck fracture. The trap is to choose internal fixation with cannulated screws because that is the answer for nondisplaced fractures. The correct answer is arthroplasty (hemiarthroplasty or total hip arthroplasty depending on functional status and acetabular condition), because the AVN rate after pinning a Garden III or IV displaced femoral neck fracture is 30 to 40 percent and the dead head will collapse. The exam scoring rule: nondisplaced = pin; displaced = replace.
The one-year mortality rate for a geriatric hip fracture is between 20 and 30 percent. Roughly one in four elderly patients who fracture a hip will literally not survive the following year. If you are a physiatrist or really any rehabilitation professional, this diagnosis demands the exact same clinical urgency as a newly discovered malignancy.
— MSK-09 podcast, ~0:00