MSK · EP 14 · SPINE
Before You Listen
Episode Setup
- Topic in one line: the bidirectional puzzle that every spine question is built around — a posterolateral disc herniation compresses the traversing nerve root (one number higher than the disc level), a far lateral or foraminal herniation compresses the exiting root, and the cervical and lumbar root-by-root maps let a clinician predict the root from the imaging or the disc from the exam.
- Prerequisites: vertebral column anatomy, basic spinal cord and nerve root anatomy, and dermatome/myotome maps for cervical and lumbar levels.
- Runtime: 1 hour 24 minutes.
Vignette. A 42-year-old construction worker reports six weeks of low back pain that radiates down the right leg into the dorsum of the foot, with numbness over the great toe. He cannot extend the great toe against resistance and the right ankle dorsiflexes weakly when tested. The patellar reflex is symmetric and the Achilles reflex is symmetric. A straight leg raise on the right reproduces radicular pain at 40 degrees of hip flexion. A magnetic resonance imaging study shows a posterolateral disc herniation at L4-L5.
Which nerve root is compressed by this herniation, why is the patellar reflex preserved, why is the Achilles reflex preserved, what is the expected sensory deficit, and what would you predict about the exam if the same patient instead had a far lateral foraminal herniation at L4-L5?
(Answer at the end of this chapter)
Section 1: The Vertebral Column, Discs, and Spinal Ligaments
Bottom line: the vertebral column has 33 vertebrae (7 cervical, 12 thoracic, 5 lumbar, 5 fused sacral, 3-5 coccygeal) and 23 intervertebral discs starting at C2-C3; the disc has a Type II collagen nucleus pulposus inside a Type I collagen annulus fibrosus and is the largest avascular structure in the body; the posterior longitudinal ligament is narrow and weak posterolaterally, which is why the vast majority of disc herniations occur in the posterolateral direction.
The human vertebral column is a segmented structure composed of 33 vertebrae arranged in five regions. The cervical spine contains 7 vertebrae, the thoracic spine 12, the lumbar spine 5, the sacrum 5 fused vertebrae, and the coccyx 3 to 5 fused segments. The vertebral column contains 23 intervertebral discs. The first disc sits between the second and third cervical vertebrae, and the last disc sits between the fifth lumbar vertebra and the first sacral segment. There is no disc between C1 and C2 because the atlantoaxial joint is a specialized rotation joint without a standard disc; the uppermost disc is at C2-C3.
The vertebral column is not straight when viewed from the side. It has four physiologic curves: the cervical lordosis (concave posteriorly), the thoracic kyphosis (convex posteriorly), the lumbar lordosis, and the sacral kyphosis. The cervical and lumbar lordotic curves are secondary curves that develop after birth in response to head control and upright posture. The thoracic and sacral kyphotic curves are primary curves present at birth.
The cervical spine has two unique vertebrae. The atlas (C1) has no vertebral body and no spinous process. It is a bony ring with anterior and posterior arches connected by lateral masses. The lateral masses articulate with the occipital condyles to form the atlanto-occipital joint, which provides approximately 50 percent of cervical flexion and extension. The axis (C2) has the odontoid process (dens), a tooth-like projection that rises vertically through the ring of the atlas and is held against the anterior arch by the transverse ligament. The atlantoaxial joint provides approximately 50 percent of cervical rotation. The transverse ligament prevents the dens from displacing posteriorly into the spinal cord. Rupture (as in rheumatoid pannus eroding the ligament) allows atlantoaxial instability with potential catastrophic spinal cord compression. The atlantodental interval, measured on a lateral radiograph between the posterior aspect of the anterior arch of the atlas and the anterior aspect of the dens, should be less than 3 mm in adults; greater than 3 mm indicates transverse ligament incompetence.
The vertebral arteries arise from the subclavian arteries and ascend through the transverse foramina of C6 to C2, then pass through the atlas (C1) separately. After exiting the transverse foramen of the atlas, they course posteriorly and medially around the lateral masses before entering the foramen magnum and joining to form the basilar artery. The vertebral arteries supply the brainstem, cerebellum, and occipital lobes; vertebral artery dissection or occlusion produces posterior circulation stroke with vertigo, diplopia, dysarthria, dysphagia, ataxia, and visual field deficits.
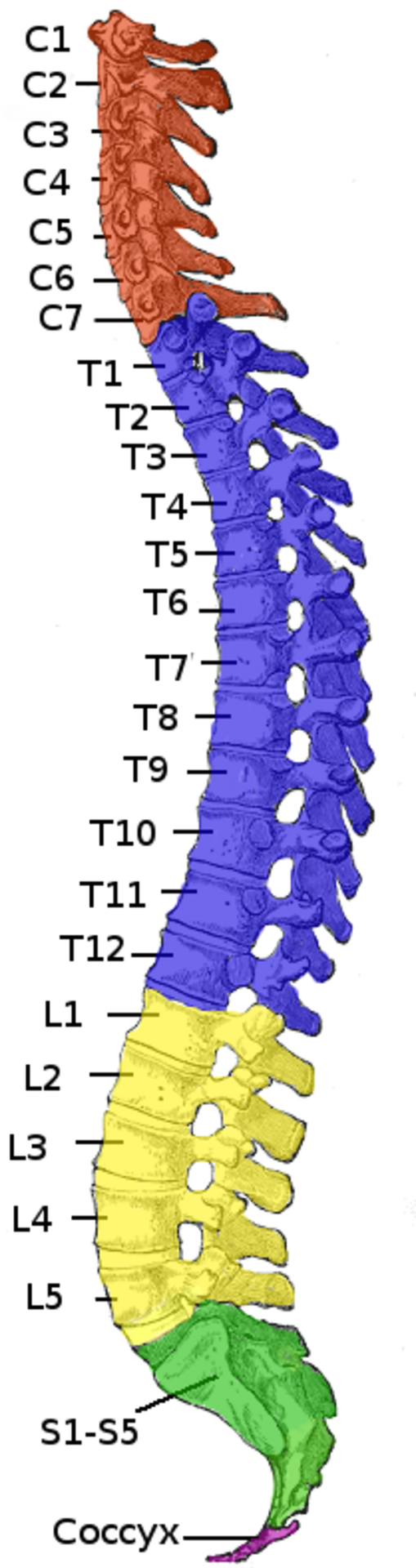
Source: Henry Vandyke Carter (Gray’s Anatomy, 1918), coloured and labelled by Uwe Gille and delldot, Wikimedia Commons, Public Domain.
The intervertebral disc is fibrocartilaginous, sits between adjacent vertebral bodies, and functions as a shock absorber, load distributor, and spacer that maintains the height of the intervertebral foramen. The nucleus pulposus is the inner core, a gelatinous, highly hydrated structure composed predominantly of Type II collagen and proteoglycans (particularly aggrecan). The high proteoglycan content gives the nucleus pulposus its water-binding capacity; in a healthy young adult it is approximately 80 to 85 percent water. When a compressive load is applied, the nucleus pulposus distributes the force evenly across the vertebral endplate and converts axial compression into radial tension on the surrounding annulus fibrosus. With aging the nucleus pulposus loses water content, becomes more fibrous, and progressively loses its ability to absorb load.
The annulus fibrosus is the outer ring, composed of concentric lamellae of Type I collagen fibers arranged in alternating oblique orientations like layers of plywood with each layer angled differently. This cross-hatched arrangement provides tremendous tensile strength and resistance to torsional forces. When the annulus develops tears or weakens with degeneration, the nucleus can herniate through the defect and compress adjacent neural structures.
The intervertebral disc is the largest avascular structure in the human body in adults. Adult discs depend on diffusion through the cartilaginous endplates from the vertebral body marrow. This avascularity has profound clinical implications: disc injuries heal poorly, disc degeneration is essentially universal with aging, and disc infections (discitis) are difficult to treat and require prolonged intravenous antibiotics.
The anterior longitudinal ligament runs along the anterior surface of the vertebral bodies from the base of the skull to the sacrum. It is the strongest spinal ligament and limits spinal extension. The posterior longitudinal ligament runs along the posterior surface of the vertebral bodies within the spinal canal. Unlike the anterior longitudinal ligament, it is narrow, thin, and relatively weak. The critical board-testable detail is that the posterior longitudinal ligament narrows as it descends through the lumbar spine and tapers laterally, leaving the posterolateral aspect of the disc relatively unsupported. This is the reason that the vast majority of disc herniations occur in the posterolateral direction; the nucleus herniates through the path of least resistance. The ligamentum flavum connects the laminae of adjacent vertebrae and forms the posterior wall of the spinal canal; its high content of elastic fibers gives it a yellow color (flavum). With aging it loses elasticity, becomes thickened and fibrotic, and buckles into the canal during extension, contributing to spinal stenosis (covered in MSK-15).
High Yield — Spine anatomy

- 33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 fused sacral, 3-5 fused coccygeal.
- 23 discs; first at C2-C3 (no disc between C1 and C2); last at L5-S1.
- Atlas (C1): no body, no spinous process; atlanto-occipital joint = 50% of cervical flex/ext.
- Axis (C2): odontoid (dens) held by transverse ligament; atlantoaxial joint = 50% of cervical rotation.
- Atlantodental interval less than 3 mm normal in adults.
- Vertebral arteries through transverse foramina C6 to C2 (then C1 separately); supply brainstem/cerebellum/occipital lobes.
- Nucleus pulposus = Type II collagen, ~80-85% water. Annulus fibrosus = Type I collagen, alternating lamellae.
- Disc is avascular in adults; nutrition by diffusion.
- Posterior longitudinal ligament is narrow and weak posterolaterally → most herniations are posterolateral.
You have this vertical peg of solid bone, the dens. So what is stopping that dens from falling backward into the neural tissue? The transverse ligament. The dens is held firmly and tightly in place against the inside of the anterior arch of the atlas by this thick critical band of connective tissue. It runs horizontally behind the dens, strapping it securely forward.
— MSK-14 podcast, ~11:22