MSK · EP 21 · RHEUM
Before You Listen
Episode Setup
- Topic in one line: the connective tissue diseases that share an autoantibody framework but split into wildly different clinical syndromes. Systemic lupus erythematosus (SLE) is the prototypical immune-complex multisystem disease; the inflammatory myopathies (dermatomyositis, polymyositis, inclusion body myositis) target proximal muscle with very different prognoses; scleroderma fibroses skin and internal organs along two distinct cutaneous patterns; and Sjögren syndrome, polymyalgia rheumatica (PMR), and giant cell arteritis (GCA) round out the connective tissue battery the boards expect on sight.
- Prerequisites: basic immunology of antinuclear antibody (ANA) testing, complement pathway activation, the type 3 hypersensitivity reaction (immune-complex deposition), creatine kinase (CK) and erythrocyte sedimentation rate (ESR) interpretation, and the proximal-versus-distal muscle anatomy from prior MSK chapters.
- Runtime: 55 minutes 10 seconds.
Vignette. A 34-year-old woman presents with fatigue, joint pain, and a facial rash. The rash is erythematous across both cheeks and over the bridge of the nose and characteristically spares the nasolabial folds. She has bilateral MCP and PIP joint swelling without erosion on radiograph. Her finger deformities resemble swan-neck deformities of rheumatoid arthritis but reduce passively to neutral. Laboratories show ANA positive at 1:1280, anti-double-stranded DNA (anti-dsDNA) positive, anti-Smith (anti-Sm) positive, low C3 and C4, urine protein-to-creatinine ratio of 1.8, and red cell casts on urine sediment.
What is the diagnosis, which serologic finding is the most specific, what does the pattern of finger deformities tell you about the underlying joint pathology, what histologic class of nephritis is most likely on biopsy, and what is the cornerstone DMARD recommended for nearly every patient with this disease?
(Answer at the end of this chapter)
Section 1: Systemic Lupus Erythematosus — Antibodies, Organs, and Jaccoud Arthropathy
Bottom line: SLE is a type 3 hypersensitivity disease driven by immune-complex deposition that hits skin, joints, kidneys, brain, and blood; ANA is sensitive (>95%) but anti-Sm is the most specific antibody; anti-dsDNA correlates with disease activity and renal flare; lupus arthritis is non-erosive and produces reducible Jaccoud deformities; and class III/IV proliferative nephritis is the leading driver of mortality.
Systemic lupus erythematosus (SLE) is a chronic, multisystem autoimmune disease driven by deposition of immune complexes in vessels and tissues, a type 3 hypersensitivity reaction. The result is systemic vascular inflammation that can attack virtually every organ. The demographic is distinctive: women of childbearing age, with a female-to-male ratio approaching 9:1, and a higher disease burden in African American, Hispanic, and Asian populations.
The 2019 European Alliance of Associations for Rheumatology (EULAR) and American College of Rheumatology (ACR) classification criteria use a positive ANA as the entry criterion. If the ANA is negative, the patient does not meet criteria. With a positive ANA, additive scoring proceeds across clinical and immunologic domains, and a total of 10 or greater establishes classification. ANA is highly sensitive (>95%) but not specific. The confirmatory antibodies are critical (Figure 21.1).

Source: CNX OpenStax (OpenStax Microbiology), Wikimedia Commons, CC BY 4.0
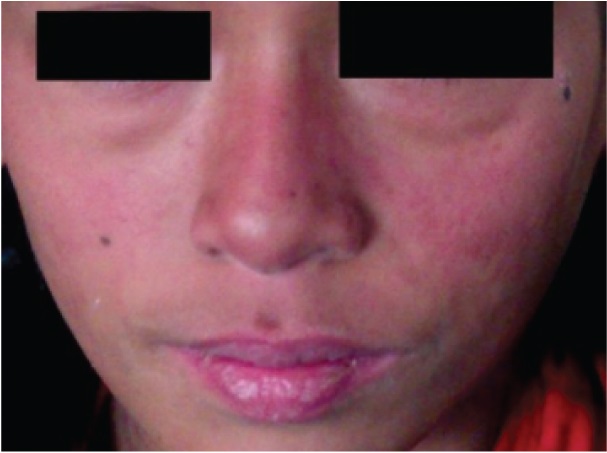
The malar (butterfly) rash is the iconic cutaneous finding: erythematous across both cheeks and over the bridge of the nose, sparing the nasolabial folds. If the erythema extends into the nasolabial creases, the diagnosis shifts toward rosacea or seborrheic dermatitis. Discoid lesions are raised, coin-shaped, erythematous plaques with adherent scaling that can cause scarring alopecia on the scalp; discoid lupus may be cutaneous-only or part of systemic disease. Photosensitivity is a hallmark, with ultraviolet exposure triggering both cutaneous flares and systemic flares (mechanism: UV-induced DNA damage and apoptosis releases nuclear material the immune system attacks). Oral ulcers occur on the hard palate and are characteristically painless, distinguishing them from the painful ulcers of Behçet disease or herpes simplex.
The arthritis of SLE is fundamentally different from rheumatoid arthritis (RA) and is high-yield for PM&R. Lupus arthritis is non-erosive. Inflammation targets synovium and periarticular soft tissues, producing ligamentous laxity rather than bony destruction. The result is Jaccoud arthropathy: ulnar deviation, swan-neck, and boutonnière deformities that look identical to advanced RA but are reducible because the bones and articular surfaces are intact (Figure 21.2). This reducibility makes splinting and orthotic interventions far more effective than in fixed RA deformities.

Serositis manifests as pleuritis (pleuritic chest pain) or pericarditis (retrosternal pain with friction rub). Pericarditis is the most common cardiac manifestation; Libman-Sacks endocarditis consists of sterile verrucous vegetations on heart valves, typically the mitral valve. Renal involvement drives morbidity and mortality. Lupus nephritis presents with proteinuria, hematuria, cellular casts, hypertension, and progressive renal insufficiency. The World Health Organization classifies it into six histologic classes; Class IV (diffuse proliferative glomerulonephritis) is the most common and most severe and demands induction therapy. Neurologic features include seizures and psychosis (both scored criteria), cognitive dysfunction, headache, mood disturbance, stroke, and peripheral neuropathy. Hematologic abnormalities include hemolytic anemia, leukopenia, lymphopenia, and thrombocytopenia.
The immunologic criteria revolve around specific antibodies and complement. Anti-double-stranded DNA (anti-dsDNA) is highly specific and tracks activity, particularly renal. Anti-Smith (anti-Sm) is the most specific antibody for SLE; it does not fluctuate with activity. Antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, anti-beta-2 glycoprotein 1) define the antiphospholipid syndrome: paradoxical hypercoagulable state with recurrent arterial and venous thromboses, recurrent fetal loss, and false-positive rapid plasma reagin (RPR) for syphilis. Despite causing thrombosis in vivo, antiphospholipid antibodies prolong the partial thromboplastin time (aPTT) in vitro, which is a classic board confusion. Complement (C3 and C4) is consumed during active disease and is depressed in flare; low complement with elevated anti-dsDNA equals active SLE.
Treatment is guided by severity. Hydroxychloroquine is the foundation of therapy and is recommended for all patients with SLE: it reduces flare frequency, protects against organ damage, and improves survival. Annual ophthalmologic screening is mandatory because of retinal toxicity. Sun protection is essential. NSAIDs treat mild musculoskeletal symptoms. Corticosteroids treat moderate-to-severe flares and organ-threatening disease. For class III or IV nephritis, induction is mycophenolate mofetil (MMF) or cyclophosphamide, with MMF preferred for its better side effect profile. Belimumab (B-lymphocyte stimulator inhibitor) is approved as add-on therapy.
Drug-induced lupus is a separate entity. The classic triggers are captured by HIP: hydralazine, isoniazid, procainamide, plus minocycline, anti-TNF agents, quinidine, methyldopa, and sulfasalazine. The serologic hallmark is anti-histone antibody in approximately 95% of cases, with anti-dsDNA and anti-Sm typically absent. Renal and neuropsychiatric involvement are uncommon, and the syndrome resolves when the offending drug is stopped.
High Yield — SLE

- ANA = sensitive screen (>95%); anti-Sm = most specific.
- Anti-dsDNA + low C3/C4 = active disease, especially renal.
- Class IV diffuse proliferative nephritis = most common and most severe.
- Jaccoud arthropathy = non-erosive, reducible deformities (splinting effective).
- Antiphospholipid syndrome = thrombosis + recurrent fetal loss + false-positive RPR + prolonged aPTT in vitro.
- Hydroxychloroquine for ALL patients; annual ophthalmologic screen for retinal toxicity.
- MMF or cyclophosphamide for class III/IV nephritis induction; belimumab as add-on.
- Drug-induced lupus = HIP (hydralazine, isoniazid, procainamide); anti-histone antibody positive.
Mnemonic — Malar rash spares the nasolabial folds
The classic SLE butterfly rash respects the nasolabial creases. If the erythema floods into the folds, think rosacea or seborrheic dermatitis, not SLE. The same logic extends to dermatomyositis: SLE rash sits between the knuckles on the proximal phalanges, and dermatomyositis (Gottron papules) sits over the knuckles themselves.
It’s essentially the bouncer at the club. A positive ANA doesn’t mean you are definitely on the VIP lupus list. It just means you are allowed to walk through the front door and be evaluated further. But a negative ANA means you are not getting in, period.
— MSK-21 podcast, ~8:39