MSK · EP 30 · SPORTS
Before You Listen
Episode Setup
- Topic in one line: the sports medicine chapters that bridge musculoskeletal medicine into general sports medicine, including hypertrophic cardiomyopathy (HCM) as the most common cause of sudden cardiac death in athletes under 35, the American Heart Association (AHA) 14-element pre-participation evaluation (PPE), Marfan syndrome with its aortic root and lens findings, commotio cordis and myocarditis, atlantoaxial instability in Down syndrome with the atlantodental interval (ADI) threshold, the wheelchair athlete shoulder as a weight-bearing joint, exercise-induced bronchospasm (EIB) with its eucapnic voluntary hyperventilation (EVH) gold-standard test, and vocal cord dysfunction (VCD) as the critical mimic of EIB.
- Prerequisites: basic cardiac auscultation (murmurs, preload-sensitive maneuvers), the autosomal dominant connective tissue disorders (Marfan, Ehlers-Danlos), the C1-C2 anatomic relationship and the transverse ligament, and the principle that exercise hyperpnea cools and dries the airways.
- Runtime: 1 hour 9 minutes.
Vignette. A 19-year-old college basketball player collapses on the court during a game. Bystander cardiopulmonary resuscitation (CPR) is initiated and an automated external defibrillator (AED) delivers one shock with return of spontaneous circulation. He is taken to the emergency department where he is stable. An echocardiogram shows asymmetric septal hypertrophy of 18 millimeters with a small left ventricular cavity and diastolic dysfunction. Family history reveals a paternal uncle who died suddenly at age 22. The patient’s 16-year-old sister is asymptomatic but is a varsity soccer player. The team physician asks two questions: what is the diagnosis and what is the immediate disposition for the patient and his sister regarding athletic participation?
What is the most likely diagnosis, what is the most common cause of sudden cardiac death in athletes under age 35 in the United States compared to athletes over age 35, what specific echocardiographic features distinguish this diagnosis from athlete’s heart, and what is the appropriate next step for the asymptomatic 16-year-old sister?
(Answer at the end of this chapter)
Section 1: Hypertrophic Cardiomyopathy and Sudden Cardiac Death
Bottom line: hypertrophic cardiomyopathy (HCM) is the most common cause of sudden cardiac death in athletes under 35 in the United States and atherosclerotic coronary artery disease (CAD) is the most common cause in athletes over 35; HCM is autosomal dominant with asymmetric septal hypertrophy 15 millimeters or greater (≥15 mm), myocardial fiber disarray, and dynamic left ventricular outflow tract obstruction; the systolic murmur of HCM increases with decreased preload (Valsalva, standing) and decreases with increased preload (squatting, leg elevation); athlete’s heart shows symmetric hypertrophy in the 13-15 millimeter range with normal diastolic function and regression after detraining.
Hypertrophic cardiomyopathy (HCM) is the number one cause of sudden cardiac death in young athletes in the United States, defined as athletes under age 35. This single fact is the most-tested cardiac sports medicine fact on the boards. HCM is an autosomal dominant genetic condition characterized by asymmetric septal hypertrophy with a septum 15 millimeters or greater (≥15 mm), myocardial fiber disarray, and dynamic left ventricular outflow tract (LVOT) obstruction.

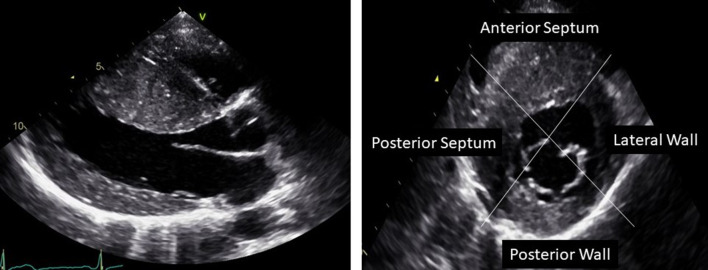
Source: Yamada T, Toyono M, et al., J Echocardiogr 2020;18:149-163, CC BY 4.0
The murmur of HCM has a distinctive and board-critical dynamic behavior. The systolic murmur increases with maneuvers that decrease preload (Valsalva, standing, dehydration), because reducing ventricular volume increases the dynamic outflow obstruction. The murmur decreases with maneuvers that increase preload (squatting, leg elevation, handgrip). This is the opposite pattern from most cardiac murmurs and is a high-yield board distinction that separates HCM from other causes of systolic murmur.
Diagnosis is confirmed by echocardiography showing septal thickness of 15 millimeters or greater (≥15 mm) with the characteristic asymmetric pattern. Athletes with confirmed HCM should be restricted from competitive sports per American College of Cardiology and AHA guidelines, though shared decision-making models have evolved in recent years.
A critical board distinction is separating HCM from athlete’s heart, because both can present with increased left ventricular wall thickness on echocardiography. Athlete’s heart shows symmetric concentric hypertrophy with wall thickness in the 13-15 millimeter range, normal diastolic function, an enlarged left ventricular cavity, and regression of the hypertrophy with detraining. HCM shows asymmetric hypertrophy predominantly affecting the septum, diastolic dysfunction, a small left ventricular cavity, and no regression with detraining. When a board question presents an athlete with borderline wall thickness, the key differentiator is whether the hypertrophy regresses after a period of deconditioning. If the wall thickness decreases after three months of detraining, it was athlete’s heart. If it persists, it is pathologic hypertrophy.
An additional high-yield fact relates to the causes of sudden cardiac death across age groups. In athletes under age 35, HCM is the leading cause. In athletes over age 35, atherosclerotic coronary artery disease (CAD) becomes the leading cause. This age-based distinction appears frequently on the boards and is one of the simplest facts to recall.
High Yield — HCM and athlete’s heart
- HCM is the number one cause of sudden cardiac death in athletes under age 35.
- Atherosclerotic CAD is the number one cause in athletes over age 35.
- HCM: autosomal dominant; asymmetric septal hypertrophy ≥15 mm; myocardial fiber disarray; dynamic LVOT obstruction.
- HCM murmur: louder with decreased preload (Valsalva, standing); softer with increased preload (squatting, leg elevation, handgrip).
- Athlete’s heart vs HCM: symmetric (13-15 mm) vs asymmetric (≥15 mm); normal vs impaired diastolic function; regresses with detraining vs no regression.
There is one specific, honestly terrifying condition that breaks this rule entirely, and it flips the physics upside down: hypertrophic cardiomyopathy. If you do things that drop ventricular volume, like having the athlete perform a Valsalva maneuver or having them stand up quickly from a squat, the murmur actually gets significantly louder. And conversely, if you do things that increase preload, like having them squat down or squeezing a handgrip to increase afterload, the murmur just fades away. That inverted paradoxical physiology is the exact reason why hypertrophic cardiomyopathy remains the number one cause of sudden cardiac death in young athletes under 35 in the United States.
— MSK-30 podcast, ~0:28