Parkinson Disease and Movement Disorders
NEURO · EP 03 · NEUROLOGY
Before You Listen
- Prerequisites: basal ganglia direct/indirect pathway anatomy and the dopamine D1/D2 receptor split; upper motor neuron vs lower motor neuron distinction (NEURO-02).
- Runtime: 38 minutes 42 seconds.
- Topic in one line: the four cardinal features of Parkinson disease (TRAP: Tremor, Rigidity, Akinesia/bradykinesia, Postural instability), the levodopa-carbidopa backbone with its motor complications, deep brain stimulation (DBS) selection criteria, the Parkinson-plus distinguishers, and the movement disorder differentials that get tested on the same vignettes: essential tremor, Huntington, dystonia, restless legs, Friedreich ataxia.
Vignette. A 64-year-old right-handed man presents with one year of progressive right-hand tremor. The tremor is most prominent when his hand rests in his lap during conversation, dissipates when he reaches for objects, and disappears in sleep. His wife reports decreased facial expression and a softer voice. On examination, you find right-greater-than-left cogwheel rigidity at the wrist, decrementing right finger-tap amplitude, normal pull test, and shortened right arm swing on gait. He has not fallen.
What is the diagnosis, the Hoehn and Yahr stage, the single highest-yield argument against an atypical parkinsonian syndrome, and the initial pharmacotherapy?
Section 1 — Pathophysiology and the TRAP Cardinal Features
Bottom line: dopaminergic loss in the substantia nigra produces TRAP (Tremor, Rigidity, Akinesia/bradykinesia, Postural instability) but bradykinesia is required for diagnosis and postural instability arrives last.
Parkinson disease is the second most common neurodegenerative disorder after Alzheimer disease, affecting approximately 1-2% over age 60. Mean onset is around 60 years, with a male predominance of roughly 3:2. About 5-10% of cases are monogenic, LRRK2, SNCA (alpha-synuclein), PARK2 (parkin), PINK1, and GBA (glucocerebrosidase) are the named genes, but the vast majority are sporadic. Advancing age is the single greatest risk factor. The cytopathological hallmark is the Lewy body, an intracytoplasmic eosinophilic inclusion composed of aggregated alpha-synuclein. By the time motor symptoms appear, 60-80% of striatal dopaminergic terminals and 50-60% of substantia nigra neurons are already gone, reflecting a long preclinical window.
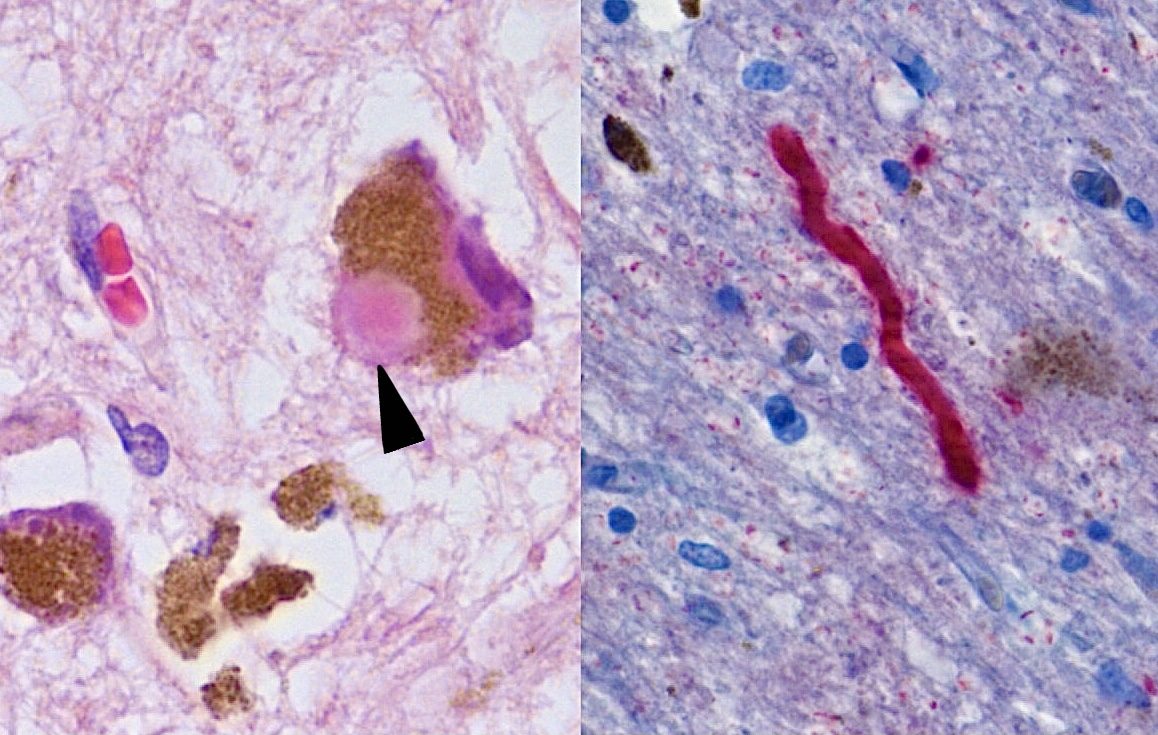
Source: Werner CJ, Heyny-von Haussen R, Mall G, Wolf S. “Proteome analysis of human substantia nigra in Parkinson’s disease.” Proteome Science 2008;6:8 (PMID 18275612). Retouched by Wikimedia user Dustfreeworld. Via Wikimedia Commons, CC BY 2.0. https://commons.wikimedia.org/wiki/File:Histological_sample_of_Substantia_nigra_in_Parkinson%27s_disease_cropped.jpg, Panel A: H&E 500× substantia nigra pars compacta neuron with intracytoplasmic Lewy body, extracellular neuromelanin, and pigment-laden macrophages. Panel B: alpha-synuclein-positive Lewy neurite at 400×.
Dopamine modulates the basal ganglia through two competing loops. The direct pathway uses D1 receptors to facilitate movement; the indirect pathway uses D2 receptors to suppress it. Dopamine depletion simultaneously underactivates the direct pathway and overactivates the indirect pathway, producing excess inhibitory output from the globus pallidus internus to the thalamus and supplementary motor area, the molecular signature of bradykinesia and rigidity. Dopamine depletion also creates relative cholinergic excess in the striatum, the rationale for the historical role of anticholinergic agents (trihexyphenidyl, benztropine) in tremor management.
The four cardinal features are remembered as TRAP: Tremor, Rigidity, Akinesia/bradykinesia, Postural instability. Postural instability is a late feature; its presence in the first year of illness is one of the strongest single arguments for an atypical syndrome rather than idiopathic Parkinson disease.


Source: Wikimedia Commons / Sir William Gowers, A Manual of Diseases of the Nervous System (1886), Public Domain.
Figure 1.1: TRAP cardinal features (reference card).
| Cardinal feature | Defining characteristics | Board distinction |
|---|---|---|
| Tremor | Resting, 4-6 Hz, “pill-rolling,” asymmetric at onset, disappears with movement and sleep | Re-emergent postural tremor returns after brief latency — still a resting tremor, NOT an action tremor |
| Rigidity | Velocity-independent resistance throughout range; lead-pipe (uniform) or cogwheel (with tremor) | Distinguishes from spasticity, which is velocity-dependent with catch-and-release |
| Akinesia/bradykinesia | Slowness + reduced amplitude + decrement on repetitive tapping; micrographia, hypomimia, hypophonia | Required for diagnosis — no bradykinesia, no Parkinson disease |
| Postural instability | Loss of postural reflexes; pull test → >2 corrective steps or examiner catch | Late feature — early prominent falls suggest progressive supranuclear palsy (PSP) |
Bradykinesia is the diagnostic linchpin. It encompasses akinesia (difficulty initiating), bradykinesia proper (slowness), and hypokinesia (reduced amplitude). On finger tapping the patient shows progressive decrement in both speed and amplitude, the same movement gets smaller and slower as it repeats. Manifestations span the body: micrographia (handwriting that shrinks across the page), masked facies (hypomimia, reduced blink rate), hypophonia (soft monotone voice), shuffling festinating gait with decreased arm swing, en-bloc turning, and the camptocormic forward trunk lean. Freezing of gait (the sudden inability to start, turn, or pass through a doorway) is a major cause of falls and tends to emerge later in the disease.
Hoehn and Yahr staging captures disease progression in five stages, with the critical transition from stage 2 to stage 3 marking the onset of postural instability and a major step-up in fall risk. Stage 1 = unilateral involvement with minimal disability; stage 2 = bilateral without balance impairment; stage 3 = bilateral with postural instability but physical independence; stage 4 = severe disability, still able to walk or stand unassisted; stage 5 = wheelchair-bound or bedridden.

The Unified Parkinson’s Disease Rating Scale (UPDRS) (or modern Movement Disorder Society UPDRS [MDS-UPDRS]) is the comprehensive clinical rating instrument with four parts: non-motor experiences of daily living, motor experiences of daily living, motor examination (the most-used in trials, scored on/off medication), and motor complications (dyskinesias and fluctuations). Diagnosis remains clinical, dopamine transporter SPECT (DAT-SPECT) is reserved for atypical or diagnostically uncertain presentations.
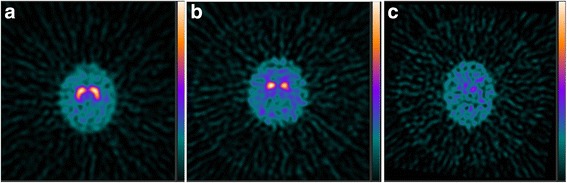
Source: Nichols KJ, Chen B, Tomas MB, Palestro CJ. “Interpreting 123I-ioflupane dopamine transporter scans using hybrid scores.” EJNMMI Research 2018;8:11. PMC5960650. Via Wikimedia Commons, CC BY 4.0. https://commons.wikimedia.org/wiki/File:Fp-cit_examples.jpg, (a) essential tremor: symmetric intense “comma-shaped” caudate + putamen uptake; (b) Parkinson disease: asymmetric putamen drop-out with relatively preserved caudate (“period/dot” pattern); (c) dementia with Lewy bodies (DLB): nearly absent caudate and putamen uptake.
Clinical Pearl — “Cogwheel rigidity equals tremor superimposed on lead-pipe”

Lead-pipe rigidity is uniform resistance; cogwheel adds the rhythmic catch of the underlying 4-6 Hz tremor breaking through. The Froment maneuver (voluntary movement of the contralateral limb) augments subtle rigidity on the tested side and is the bedside trick for unmasking early disease.
Board Trap — “Asymmetric onset means atypical”

Wrong direction: idiopathic Parkinson disease is classically asymmetric at onset, and symmetric presentation is what should raise suspicion for a Parkinson-plus syndrome (PSP, multiple system atrophy [MSA]).
High Yield — TRAP in 5 lines

- Tremor: resting, 4-6 Hz, pill-rolling, asymmetric, disappears with movement.
- Rigidity: velocity-INDEPENDENT (vs spasticity); cogwheel = tremor + lead-pipe.
- Akinesia/bradykinesia: required for diagnosis; decrementing finger taps.
- Postural instability: late: early falls suggest PSP, not PD.
- Pathology: substantia nigra dopaminergic loss + alpha-synuclein Lewy bodies.
You sit down, you describe these tiny annoyances, and the physician looks at you and tells you that somewhere between 60% to 80% of the dopamine-producing terminals in your brain are already dead, permanently gone. The disease has been quietly destroying the architecture of the brain for years, perhaps even decades, before that patient ever notices their hand shaking.
— NEURO-03 podcast, ~00:24