PEDS · EP 03 · SPINABIFIDA
Before You Listen
Episode Setup
- Topic in one line: the whole arc of spinal dysraphism in one sitting — neural tube closure by day 28 post-conception driving preconceptional folic acid (0.4 mg general; 4 mg with a prior neural tube defect (NTD) pregnancy); the spectrum from spina bifida occulta through closed lipomyelomeningocele to open meningocele and myelomeningocele (the most clinically significant form, ~90 percent of treatment-requiring live-born NTDs); maternal serum alpha-fetoprotein (MSAFP) plus amniocentesis acetylcholinesterase (AChE) plus the ultrasound lemon and banana signs for prenatal diagnosis; the Management of Myelomeningocele Study (MOMS) trial showing that prenatal repair halves the ventriculoperitoneal (VP) shunt rate; the Arnold-Chiari II malformation with infant brainstem compression as the most life-threatening early presentation; tethered cord as a clinical (not radiographic) diagnosis driven by progressive change; the functional motor levels that determine ambulation prognosis (L4 plus tibialis anterior is the classic ankle-foot orthosis community ambulator); neurogenic bladder protection through clean intermittent catheterization and the McGuire 40 cm H₂O detrusor leak point pressure threshold; neurogenic bowel culminating in the Malone antegrade continence enema (MACE) procedure; latex precautions using the BACK food list (Banana, Avocado, Chestnut, Kiwi); and the orthopedic philosophy that contrasts sharply with cerebral palsy because hip reduction in spina bifida does not improve ambulation.
- Prerequisites: the basics of embryology (anterior versus posterior neuropore), the difference between Chiari I and Chiari II, the framework of hydrocephalus and shunt physiology, the spinal cord level-to-muscle map, and the upper-versus-lower motor neuron bladder and bowel framework.
- Runtime: to be confirmed after the episode re-fire.
Vignette. A 2-day-old neonate is born with a 4 cm lumbosacral skin defect, exposed neural tissue, and absent voluntary motion below the knees. Prenatal ultrasound at 20 weeks showed the lemon and banana signs. Maternal serum alpha-fetoprotein was 4.2 multiples of the median at 16 weeks. Postnatal exam shows quadriceps strength 4/5 bilaterally, absent ankle dorsiflexion, and absent foot intrinsics. The neonate has a tense anterior fontanelle, increasing head circumference, and weak cry with intermittent stridor. Renal ultrasound reveals mild bilateral hydronephrosis.
What did the prenatal ultrasound and MSAFP tell us about the lesion, what is the functional motor level, what is the most likely cause of the head circumference change, what is the most life-threatening current finding, what bladder management must begin now, and what is the long-term prognosis for community ambulation?
(Answer at the end of this chapter)
Section 1: Neural Tube Closure, Folic Acid, and the Open-Versus-Closed Rule
Bottom line: the neural tube closes by day 28 post-conception (anterior neuropore day 25, posterior neuropore day 27 to 28), often before a woman knows she is pregnant. Folic acid supplementation must therefore begin preconceptionally: 0.4 mg daily for all women of childbearing age, 4 mg daily for women with a prior NTD-affected pregnancy. United States mandatory grain fortification (1998) reduced NTD prevalence by approximately 26 to 28 percent. Valproic acid is the most teratogenic commonly used antiepileptic drug (10 to 20x baseline risk). The lesion spectrum runs from spina bifida occulta (incidental vertebral arch defect, 5-10 percent of the general population) through closed lipomyelomeningocele (no exposed tissue but tethered cord risk) to open meningocele (meninges only) and myelomeningocele (meninges plus exposed neural tissue, ~90 percent of treatment-requiring NTDs). Open NTDs elevate MSAFP; closed dysraphisms do not.
The neural tube forms by fusion of the neural folds during the third and fourth weeks of embryonic development. The anterior neuropore closes by day 25 post-conception and the posterior neuropore by day 27 to 28. Failure of posterior neuropore closure produces myelomeningocele; failure of anterior closure produces anencephaly. Because the entire process is complete before the first missed menstrual period, prevention must begin preconceptionally at the population level. This is a fixed biological constraint, not a behavioral one. A woman who learns she is pregnant at 6 weeks and immediately starts folic acid has missed the window by a full month.
Epidemiology. United States NTD prevalence is approximately 0.5 to 0.7 per 1000 live births, down from approximately 1.0 to 1.5 per 1000 before mandatory folic acid grain fortification began in 1998. Worldwide prevalence ranges from 0.5 to 2.0 per 1000 by region, ethnicity, and dietary practice. Myelomeningocele accounts for approximately 90 percent of live-born NTDs that require postnatal treatment. Anencephaly is the other major contributor but is incompatible with life and so is rarely seen on rehabilitation wards. Sex distribution is roughly equal, with a slight female predominance.
Folate prevention: the evidence base. The Medical Research Council Vitamin Study (Lancet 1991) was a randomized controlled trial demonstrating a 72 percent reduction in NTD recurrence with 4 mg folic acid daily in women with a prior NTD pregnancy. Czeizel and Dudas (NEJM 1992) extended that finding by demonstrating that folic acid prevents first-occurrence NTDs as well. Together these two trials established the dosing standard. The recommended doses are 0.4 mg (400 mcg) daily for all women of childbearing age (ongoing, preconceptional, lifelong) and 4 mg daily for women with a prior NTD-affected pregnancy (start 1 to 3 months before conception and continue through the first trimester). United States mandatory grain fortification since 1998 has reduced NTD prevalence by approximately 26 to 28 percent in the general population, a smaller relative effect than the 72 percent seen in supplemented high-risk individuals because dietary intake from fortification is modest.
Risk factors for NTDs. Prior NTD-affected pregnancy carries a recurrence risk of 2 to 5 percent (10 to 20-fold the population baseline); two affected siblings push the risk to approximately 10 percent. Other major risk factors include maternal folate deficiency (the primary modifiable risk factor), maternal diabetes (2 to 10x baseline), maternal obesity (1.5 to 3.5x baseline), maternal first-trimester hyperthermia (febrile illness or hot tub exposure), and several teratogenic medications. Valproic acid carries a 1 to 2 percent NTD risk (10 to 20x baseline) and is the most teratogenic commonly used antiepileptic drug. Carbamazepine carries a 0.5 to 1 percent risk. Folic acid antagonists (methotrexate, trimethoprim, aminopterin) also raise risk. Hispanic ethnicity and lower socioeconomic status are independent epidemiologic associations, likely mediated by dietary folate intake and access to prenatal care.
The clinical implication for the rehabilitation physician is direct: any woman of childbearing age on valproic acid for spasticity, headache, or seizure deserves explicit preconceptional counseling, a 4 mg folic acid prescription if she might become pregnant, and frank discussion of switching to a less teratogenic agent (lamotrigine or levetiracetam) when feasible. This conversation belongs in the rehabilitation clinic, not just the obstetrician’s office.
Why fortification works. Mandatory grain fortification (140 mcg folic acid per 100 g of enriched cereal grain in the United States since January 1998) operates as a population-level intervention precisely because it bypasses the behavioral problem. A woman who plans a pregnancy and takes prenatal vitamins is already in the lowest-risk group; the women who benefit most from fortification are those whose pregnancies are unplanned or who first present for care after the neuropore has already closed. The 26 to 28 percent reduction is the residual benefit captured even when no intentional supplementation occurs, and it has been replicated in dozens of countries that have adopted similar fortification policies. Conversely, countries without fortification continue to see NTD rates 2 to 3 times higher than the United States.
High Yield — Embryology and prevention

- Neural tube closes by day 28 post-conception (anterior neuropore day 25; posterior day 27-28).
- Folic acid must be preconceptional: 0.4 mg daily for all women of childbearing age; 4 mg daily for prior NTD pregnancy (start 1-3 months pre-conception through first trimester).
- US grain fortification (1998) dropped NTD prevalence ~26-28 percent.
- MRC Vitamin Study (Lancet 1991) = 72 percent reduction in recurrence with 4 mg folic acid; Czeizel and Dudas (NEJM 1992) extended to first-occurrence prevention.
- Valproic acid = the most teratogenic common antiepileptic drug (1-2 percent NTD risk, 10-20x baseline).
- Recurrence risk after one affected pregnancy: 2-5 percent; two affected siblings: ~10 percent.
- Maternal diabetes, obesity, first-trimester hyperthermia, methotrexate, trimethoprim all raise risk.
Spina bifida occulta is a posterior vertebral arch defect without neural tissue involvement. It is present in 5 to 10 percent of the general population as an incidental radiographic finding, is usually asymptomatic, and does not elevate MSAFP. The clinical task is to recognize it as benign in most cases while screening for the rare occult tethered cord that can hide beneath it.
Lipomyelomeningocele is the most common closed dysraphism: a lipoma adherent to the spinal cord through a posterior vertebral defect with intact overlying skin. There is no exposed neural tissue, and MSAFP is normal because nothing is leaking into the amniotic fluid. The closed surface, however, does not mean closed risk: the lipomatous tether places these patients at lifelong risk for symptomatic tethered cord requiring surgical release. Cutaneous markers (hairy patch, subcutaneous lipoma, dimple) typically betray the diagnosis on the newborn skin exam.
Meningocele is herniation of meninges only, without neural tissue, through a posterior vertebral defect. It accounts for approximately 5 percent of NTDs, elevates MSAFP because meningeal sac fluid communicates with the amniotic environment, and carries a substantially better prognosis than myelomeningocele because the spinal cord itself is structurally intact within the canal.
Myelomeningocele is herniation of both meninges and neural tissue through a posterior vertebral defect with the placode of dysplastic spinal cord exposed at the surface. It elevates MSAFP markedly. It accounts for approximately 90 percent of treatment-requiring live-born NTDs, and it is the lesion every remaining section of this chapter is built around.
Anencephaly results from failure of anterior neural tube closure. It accounts for approximately 50 percent of all NTDs but is incompatible with life beyond a few hours to days; it is included for completeness on the embryology spectrum, not for clinical management.
Encephalocele is a brain herniation through a skull defect, usually occipital, with variable prognosis depending on the volume and location of herniated brain tissue.
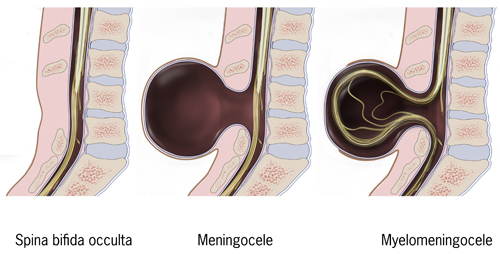
Source: Wikimedia Commons, “Typesofspinabifida” (public domain illustration).
Cutaneous markers of closed dysraphism above the gluteal cleft include a hairy patch, sacral dimple above the gluteal cleft (dimples below the gluteal cleft are usually benign pilonidal pits), hemangioma, dermal sinus tract, subcutaneous lipoma, and skin appendage. Any of these cutaneous stigmata over the lumbosacral spine warrants imaging (typically ultrasound in the neonate and MRI thereafter), even when the neurological examination is entirely normal. This is the screen that catches the lipomyelomeningocele that would otherwise present years later as a symptomatic tethered cord.
The open-versus-closed distinction is the highest-yield concept of this section. Open NTDs (myelomeningocele, anencephaly, meningocele) have exposed or surface-near neural tissue and therefore elevate MSAFP. Closed dysraphisms (lipomyelomeningocele, spina bifida occulta) have intact skin and do NOT elevate MSAFP. A normal MSAFP does not exclude a closed dysraphism, and that limitation is a frequently tested distractor.
High Yield — Types and the open-closed distinction
- Spina bifida occulta = posterior vertebral arch defect; 5-10 percent of general population; usually incidental; normal MSAFP.
- Lipomyelomeningocele = closed dysraphism with lipoma adherent to cord; intact skin; normal MSAFP; tethered cord risk.
- Meningocele = meninges only; ~5 percent of NTDs; MSAFP elevated; better prognosis.
- Myelomeningocele = meninges + exposed neural tissue; ~90 percent of treatment-requiring NTDs; MSAFP elevated.
- Cutaneous markers above the gluteal cleft (hairy patch, dimple, hemangioma, sinus tract, lipoma) require imaging even with normal exam.
- Open NTDs elevate MSAFP; closed dysraphisms do NOT (the frequently tested distinction).
Mnemonic — “OPEN raises AFP; CLOSED hides”
Open NTDs (myelomeningocele, meningocele, anencephaly) have exposed or surface-near neural tissue, so amniotic alpha-fetoprotein leaks freely and MSAFP rises. Closed dysraphisms (lipomyelomeningocele, occulta) have intact skin, so MSAFP is normal and the diagnosis is made by cutaneous stigmata plus imaging, not serum screening. A normal MSAFP never excludes a closed defect.