PEDS · EP 05 · BRACHIAL
Before You Listen
Episode Setup
- Topic in one line: the obstetric stretch injury to the C5-T1 brachial plexus that produces the “waiter’s tip” of upper plexus Erb-Duchenne palsy, the rare claw hand and Horner syndrome of lower plexus Klumpke palsy, and the flail-arm total plexopathy whose recovery trajectory is decided in the first six months by serial Active Movement Scale (AMS) examinations, the Toronto Test Score, and the Cookie Test.
- Prerequisites: brachial plexus anatomy from roots through terminal branches (covered in MSK-03 and EDX-07), Seddon-Sunderland nerve injury classification (EDX-01), and the dorsal root ganglion (DRG) localization rule that preserves sensory nerve action potentials (SNAPs) in preganglionic root avulsion despite clinical numbness.
- Runtime: 58 minutes.
Vignette. A 4,300-gram boy is delivered vaginally after a prolonged second stage with documented shoulder dystocia. On day 1 of life, the right arm hangs limply at the infant’s side, internally rotated and pronated, the elbow extended, the wrist flexed. The Moro reflex is absent on the right, and the right palmar grasp is preserved and brisk. Pupils are equal and reactive. A right clavicle fracture is noted on chest radiograph. At a 1-month follow-up the deltoid and biceps remain non-functional, although finger flexion is full strength.
What is the brachial plexus injury pattern, what is the prognostic significance of the preserved hand grip and the absence of Horner syndrome, what assessment tool is used at 3 months to decide on microsurgery, and what nerve transfer is most commonly used to restore biceps function in this child?
(Answer at the end of this chapter)
Section 1: Plexus Anatomy and the Mechanics of Birth Injury
Bottom line: the brachial plexus runs C5-T1 through three trunks, six divisions, three cords, and five terminal branches; lateral neck-shoulder traction during shoulder dystocia or breech extraction stretches the upper plexus and produces Erb-Duchenne palsy in 70-80% of birth injuries; macrosomia greater than 4 kilograms and shoulder dystocia raise the risk roughly 100-fold, and the dorsal root ganglion localization principle separates preganglionic root avulsion (SNAP preserved despite numbness) from postganglionic rupture or stretch.
The brachial plexus is built from the ventral rami of spinal nerve roots C5, C6, C7, C8, and T1. The roots converge to form three trunks: the upper trunk from C5 plus C6, the middle trunk from C7 alone, and the lower trunk from C8 plus T1. Each trunk splits into anterior and posterior divisions, producing six divisions, which recombine to form three cords named for their relationship to the axillary artery. The lateral cord receives the anterior divisions of the upper and middle trunks; the posterior cord receives all three posterior divisions; the medial cord receives the anterior division of the lower trunk. The cords give rise to the five major terminal branches: musculocutaneous, axillary, radial, median, and ulnar.
Several proximal branches arise before the cords and matter for localization. The dorsal scapular nerve (C5 root) supplies the rhomboids; rhomboid weakness localizes injury proximal to the trunk and signals possible root avulsion. The long thoracic nerve (C5, C6, C7 roots) supplies the serratus anterior; injury produces medial scapular winging. The suprascapular nerve (upper trunk) supplies the supraspinatus and infraspinatus; this is the workhorse abductor and external rotator that fails in Erb palsy. The phrenic nerve (C3, C4, C5 roots) supplies the diaphragm; ipsilateral hemidiaphragm paralysis on chest radiograph occurs in approximately 5 percent of brachial plexus birth injuries and is more common with total palsy.
The mechanism of birth injury is lateral traction that separates the head from the shoulder. In vertex deliveries, lateral pull on the head away from the impacted shoulder stretches the upper plexus and produces the Erb-Duchenne pattern. In breech deliveries, lateral traction on the trunk and arms preferentially stretches the lower plexus, although upper plexus injuries still predominate overall. The severity of stretch determines whether the lesion is a focal demyelinating neurapraxia with full recovery, an axonotmesis with axonal disruption and variable recovery, or a root avulsion in which the rootlet is torn from the spinal cord with no potential for spontaneous recovery.

Source: Adapted from open-source brachial plexus diagram (Wikimedia Commons / public domain).
The strongest single risk factor is shoulder dystocia, which raises injury risk roughly 100-fold and is documented in approximately 50 percent of cases. Macrosomia above 4,000 grams (and especially above 4,500 grams) increases risk 4 to 14-fold, often through maternal diabetes. Other contributors include forceps or vacuum extraction, prolonged second stage, breech presentation (particularly for lower plexus patterns), multiparity, and a previously affected sibling (recurrence risk approximately 5-15%). Two medicolegally important caveats: roughly 50 percent of cases occur without documented shoulder dystocia, and 1-4 percent occur after cesarean delivery, indicating that intrauterine positioning and forces can also contribute. The most commonly associated injury is an ipsilateral clavicle fracture (10-15%), which may actually be protective by absorbing energy that would otherwise reach the plexus.
Board answer vs. current evidence — Shoulder dystocia is the strongest risk factor and raises brachial plexus birth injury risk roughly 100-fold — this is likely the board-tested answer, but more recent evidence (PMID 32501916) indicates the exact magnitude of the risk increase from shoulder dystocia remains uncertain, with reported estimates varying widely across populations. Answer the board-canonical version on the test.
The DRG localization rule drives every electrodiagnostic study in this chapter. The dorsal root ganglion sits inside the intervertebral foramen, outside the spinal cord. A root avulsion is preganglionic: the rootlet is torn from the cord, but the DRG remains continuous with the peripheral sensory axon, so the SNAP is preserved despite clinical numbness. A root rupture is postganglionic: the DRG is separated from its central axon, the peripheral axon undergoes Wallerian degeneration, and the SNAP is reduced or absent. A clinically numb infant with preserved SNAPs in that dermatome has avulsion until proven otherwise. Imaging signs of avulsion include a pseudomeningocele on magnetic resonance imaging (MRI) of the cervical spine, with clinical accompaniments of Horner syndrome (T1), elevated hemidiaphragm (phrenic), scapular winging (long thoracic), and rhomboid weakness (dorsal scapular).
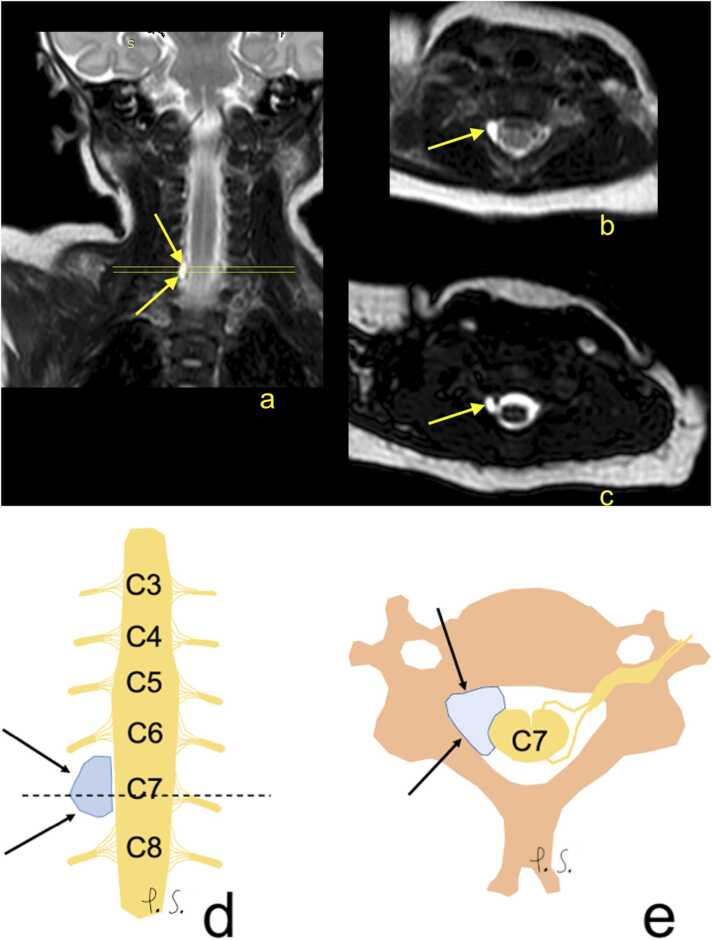
Source: Somashekar DK, et al. “Magnetic resonance imaging of the brachial plexus. Part 2: Traumatic injuries.” European Journal of Radiology Open 2022;9:100397. CC BY 4.0.
High Yield — Anatomy and risk

- Plexus map: C5-T1 → 3 trunks (upper C5-C6, middle C7, lower C8-T1) → 6 divisions → 3 cords (lateral, posterior, medial) → 5 terminal branches (musculocutaneous, axillary, radial, median, ulnar).
- Proximal branches that localize injury: dorsal scapular C5 (rhomboids), long thoracic C5-C7 (serratus → winging), suprascapular upper trunk (supra/infraspinatus), phrenic C3-C5 (diaphragm).
- Strongest risk factor: shoulder dystocia (~100x risk), present in ~50% of cases. Macrosomia >4 kg (OR 4-14x).
- ~50% of cases occur without documented shoulder dystocia; 1-4% occur after cesarean.
- Most common associated injury: ipsilateral clavicle fracture (10-15%), possibly protective.
- Preganglionic avulsion = SNAP preserved despite numbness; pseudomeningocele on MRI.
- Postganglionic rupture/stretch = SNAP reduced or absent.
Mnemonic — “Read That Damn Cadaver Book”

The five layers of the plexus from proximal to distal: Roots → Trunks → Divisions → Cords → Branches. Roots (C5-T1), Trunks (upper, middle, lower), Divisions (3 anterior + 3 posterior), Cords (lateral, posterior, medial), terminal Branches (musculocutaneous, axillary, radial, median, ulnar).
It acts exactly like a mechanical fuse in an electrical circuit. If the clavicle breaks, the bone absorbs that kinetic energy as it snaps. So, paradoxically, a broken clavicle often means the nerve injury is less severe than it could have been.
— PEDS-05 podcast, ~31:24