PEDS · EP 09 · MSK
Before You Listen
Episode Setup
- Topic in one line: the pediatric musculoskeletal disorders that earn their own ABPMR Part I vignettes, including developmental dysplasia of the hip (DDH), Legg-Calvé-Perthes disease (LCPD), slipped capital femoral epiphysis (SCFE), the Salter-Harris (SH) physeal fracture grades, the apophysitis family, a small set of high-risk pediatric forearm and elbow injuries, adolescent idiopathic scoliosis (AIS), clubfoot, congenital muscular torticollis (CMT), and osteogenesis imperfecta (OI).
- Prerequisites: general orthopedic vocabulary (varus, valgus, abduction, adduction, rotation), basic pediatric growth physiology (physis = growth plate; apophysis = secondary ossification center at a tendon insertion), and the limb examination framework from PEDS-01. Memorize them cold.
- Runtime: 1 hour 5 minutes.
Vignette. A 12-year-old boy with a body mass index in the 95th percentile reports four weeks of a dull ache in the left medial thigh and knee. He denies trauma. He walks with the left foot turned out. On examination, when the examiner attempts to flex the left hip, the leg drifts into obligatory external rotation. Internal rotation and abduction are limited and painful. Knee examination is unremarkable. Plain radiographs of the bilateral knees are normal.
What is the most likely diagnosis, what radiographic study and view will confirm it, what radiographic line is used to make the diagnosis, what is the appropriate next step in management, and what is one critical management pitfall the treating team must avoid?
(Answer at the end of this chapter)
Section 1: The Pediatric Hip — DDH, LCPD, and SCFE by Age Window
Bottom line: three hip disorders dominate pediatric orthopedic vignettes, each defined by an age window. Developmental dysplasia of the hip (DDH) sits in the newborn and infant. Legg-Calvé-Perthes disease (LCPD) appears in the 4 to 10 year old (peak 5 to 7, male predominance, Herring lateral pillar grade drives prognosis). Slipped capital femoral epiphysis (SCFE) shows up in the 10 to 16 year old (classically the obese adolescent boy with knee or thigh pain whose radiograph shows the femoral head slipping off the metaphysis like ice cream off a cone).
The pediatric hip yields a disproportionate share of board questions because the same chief complaint of limp or hip pain points at completely different pathology in three age windows. The first move on every stem is to pin down the patient’s age, then narrow the differential by sex, body habitus, and a single radiographic finding. A useful framing is that the same hip can fail in three mechanical ways depending on which structure is still maturing: the acetabulum in DDH, the vascular supply to the capital epiphysis in LCPD, and the proximal femoral physis in SCFE.
Developmental dysplasia of the hip (DDH) spans mild acetabular dysplasia to frank dislocation. It affects 1 to 2 per 1,000 live births for dislocation and 10 to 20 per 1,000 for instability or dysplasia overall. The female-to-male ratio is 4:1 to 8:1, and the left hip carries 60% of cases because the most common fetal position (left occiput anterior) presses the left hip against the maternal sacrum. Highest-priority risk factors are breech presentation, female sex, firstborn status, positive family history, and oligohydramnios. The Barlow test (hip flexed 90 degrees, gentle adduction with a posterior force) dislocates a dislocatable hip; the Ortolani test (hip flexed 90 degrees, gentle abduction with an anterior lift) reduces a dislocated hip with a palpable clunk. The mnemonic is “Barlow is Bad” because it is provocative, and “Ortolani is OK” because it is reductive. The Galeazzi sign (unequal knee heights with both hips and knees flexed) points to unilateral dislocation. Asymmetric skin folds appear in roughly 25% of normal infants and are suggestive but not diagnostic.
Imaging follows a strict age rule. Ultrasound is preferred before 4 to 6 months because the femoral head is largely cartilaginous, and radiographs become useful only after the ossific nucleus appears. The Graf classification grades the alpha angle: Type I greater than 60 degrees (normal); Type IIa 50 to 59 degrees in an infant under 3 months (physiologic immaturity); Type IIb 50 to 59 degrees in an infant over 3 months (delayed ossification, treat); Type IIc 43 to 49 degrees (critical zone, significant dysplasia); Type III under 43 degrees (subluxated); Type IV (dislocated). The Pavlik harness is first-line treatment before 6 months at 100 to 110 degrees of flexion and less than 70 degrees of abduction; success rates run 85% to 95%. Forced abduction beyond 70 degrees raises avascular necrosis (AVN) risk, and the harness is contraindicated after 6 months, in teratologic dislocations, or after a 3- to 4-week trial fails. Closed reduction with hip spica casting follows Pavlik failure; open reduction is reserved for hips that will not concentrically reduce, typically presenting after 12 to 18 months. Untreated dislocation leads to progressive acetabular deformation, an abnormal gait, and premature osteoarthritis.

Legg-Calvé-Perthes disease (LCPD) is idiopathic osteonecrosis of the femoral head in children aged 4 to 10 years (peak 5 to 7). Incidence is roughly 1 in 1,200 children; the M:F ratio is 4:1 to 5:1; bilateral involvement runs 10% to 15% and is usually asynchronous. Bilateral synchronous disease should trigger an endocrine workup for hypothyroidism, growth hormone deficiency, or skeletal dysplasia, because true synchronous bilateral Perthes is rare and often points at a systemic cause. The Waldenström stages run from initial (necrosis, increased femoral head density, widened joint space), to fragmentation (mixed lytic and sclerotic), to reossification, to remodeling. The Herring lateral pillar classification, taken at the fragmentation stage, is the most powerful prognosticator: Group A (full height, good); Group B (>50%, intermediate); Group B/C (~50%, guarded); Group C (<50%, poor). The Stulberg classification scores the final femoral head shape at skeletal maturity, from I (spherical, good) to V (flat head with normal acetabulum, poor with early arthritis).
Age at onset is the single strongest prognostic factor: children younger than 6 do well regardless of Herring grade; children older than 8 with Group B/C or C disease typically need surgical containment via femoral or pelvic osteotomy. “Head at risk” radiographic signs include the Gage sign (a V-shaped lucency on the lateral epiphysis), calcification lateral to the epiphysis, lateral subluxation, and a horizontal physis. Containment (abduction bracing or surgical osteotomy) lets the acetabulum mold the softened head into a spherical form during reossification. Initial management of the painful Perthes hip is rest, protected weight-bearing, range of motion, and NSAIDs as needed for symptom relief.

Source: Wikimedia Commons / open-source pediatric radiology atlas (PD or CC BY).
Slipped capital femoral epiphysis (SCFE) is the most common adolescent hip disorder, incidence 10.8 per 100,000. The classic patient is an overweight adolescent boy aged 10 to 16. Additional risk factors include African American race, hypothyroidism, growth hormone therapy, and renal osteodystrophy. Bilateral involvement is 18% to 50%. The mechanism is failure of the hypertrophic zone of the physis under shear stress; the epiphysis displaces posteriorly and inferiorly while the metaphysis moves anteriorly and superiorly. Patients walk with an antalgic gait and externally rotated leg, complain of knee or medial thigh pain (the classic referral pattern that traps unwary clinicians), and demonstrate obligatory external rotation when the examiner flexes the hip (the Drehmann sign). Internal rotation and abduction are limited.
Any adolescent with knee or thigh pain deserves hip radiographs; the frog-leg lateral is the most sensitive view because mild posterior slips become obvious in flexion-abduction. The diagnostic finding is the Klein line, drawn along the superior femoral neck, which fails to intersect the femoral head once the epiphysis slips. The Loder classification splits SCFE by stability: stable SCFE (can bear weight) carries an AVN risk of 0% to 10%; unstable SCFE (cannot bear weight) carries an AVN risk of 24% to 47%. Treatment for stable SCFE is in situ percutaneous single-screw fixation. Do not reduce the slip; forced reduction crushes the already tenuous retinacular blood supply along the femoral neck. Unstable SCFE is an orthopedic emergency requiring urgent operative stabilization. Bilateral prophylactic fixation is favored in patients younger than 10, those with endocrine risk factors, and those with bilateral abnormalities at presentation.
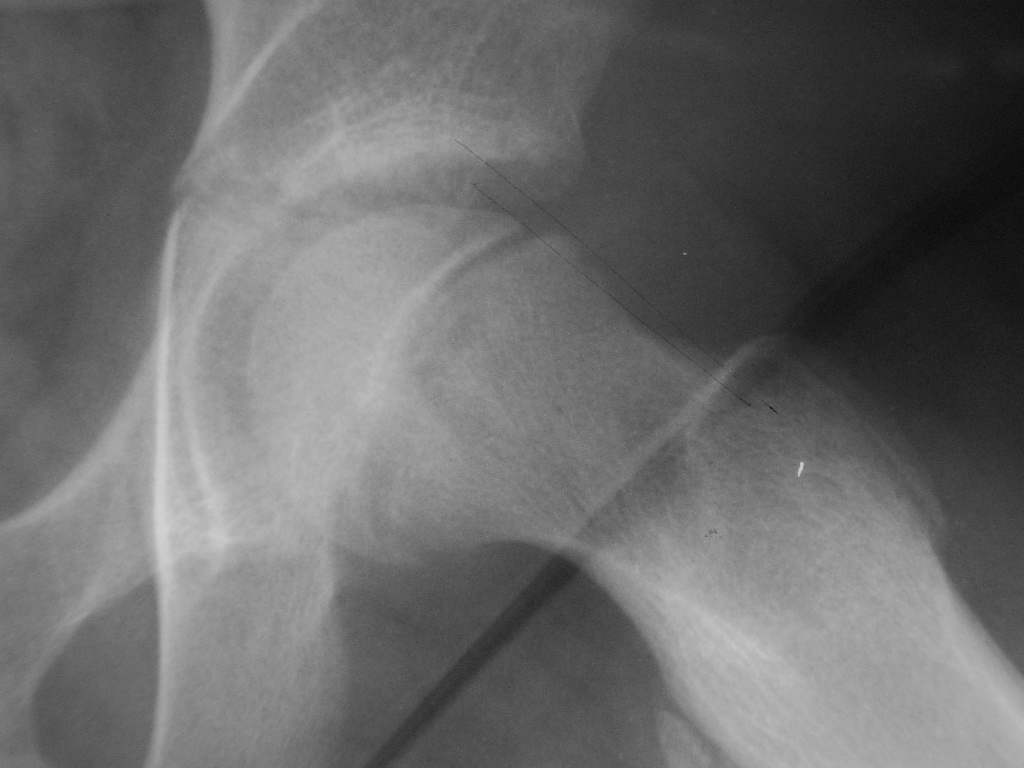
Source: Wikimedia Commons / Radiopaedia (PD or CC BY).
High Yield — The pediatric hip triad
- DDH = newborn/infant; F >> M; left hip 60%; Barlow dislocates, Ortolani reduces; ultrasound before 4-6 months, then radiographs; Pavlik harness before 6 months at 100-110 deg flexion / <70 deg abduction; success 85-95%.
- Graf classification: Type I >60 deg (normal); IIc 43-49 deg (critical); III <43 deg (subluxated); IV (dislocated).
- LCPD = ages 4-10, peak 5-7; M:F 4-5:1; bilateral 10-15% (consider endocrine workup if synchronous); Herring lateral pillar A / B / B-C / C is the single most useful prognostic grade; age <6 does well regardless.
- SCFE = 10-16 yo, obese, M > F; knee or medial thigh pain with obligatory external rotation on hip flexion (Drehmann); Klein line on frog-leg lateral fails to intersect the head; in situ single-screw fixation; do NOT reduce a stable slip.
- Unstable SCFE = cannot bear weight = AVN 24-47% = orthopedic emergency.
Mnemonic — Hip pain by age window

- 0-6 months: DDH (Barlow/Ortolani; ultrasound; Pavlik).
- 3-8 years: transient synovitis (post-viral, self-limited) vs septic arthritis (Kocher criteria; see PEDS-10).
- 4-10 years: LCPD (Herring grade).
- 10-16 years: SCFE (Klein line).
Board Trap — “Just a knee sprain”

A heavyset 13-year-old presents with a four-week limp and medial thigh or knee pain. The trap is to image the knee, find nothing, and discharge with a knee brace. The correct move (in clinic and on the test) is dedicated hip radiographs (AP pelvis plus frog-leg lateral) every time. Knee pain in an adolescent is an SCFE until the Klein line proves otherwise.
The classic radiographic diagnostic tool is Klein’s line. You draw a perfectly straight line extending along the superior edge of the femoral neck. In a normal healthy hip, that line should pass through and intersect a small portion of the lateral femoral head. But in an SCFE patient, the Klein’s line will pass completely outside the head, failing to intersect it at all. The visual analogy that everyone uses, and it is perfectly accurate, is a scoop of ice cream slipping backward off an ice cream cone.
— PEDS-09-a podcast, ~46:58