PEDS · EP 11 · BURNS
Before You Listen
Episode Setup
- Topic in one line: the pediatric burn vignette that drives ABPMR Part I questions: the Lund-Browder chart for age-adjusted total body surface area (TBSA), the modified rule of nines, burn depth and its inverse relationship to pain, the Parkland formula with its pediatric dextrose modification, Jackson’s three burn zones, anti-deformity positioning (the “comfort equals contracture” doctrine), the dorsal hand “safe / intrinsic plus” position, pressure garments and scar management, and the non-accidental trauma (NAT) pattern recognition built around stocking distribution, doughnut sign, flexion-crease sparing, and delay greater than 2 hours.
- Prerequisites: general burn vocabulary (depth classification, eschar, escharotomy), basic peripheral nerve and muscle anatomy of the hand (intrinsics, MCP / IP joints, collateral ligaments), and the rehabilitation framework from MEDREH for splinting and positioning.
- Runtime: approximately 30 minutes for Part 1.
- Scope boundary: Part 1 covers pediatric burns end-to-end (assessment, resuscitation, rehabilitation, NAT). Part 2 pivots to the pediatric oncology and hematology content: posterior-fossa brain tumors, ALL versus AML, neuroblastoma, Wilms, rhabdomyosarcoma, the Van Ness rotationplasty, sickle cell disease, cancer-related fatigue, and the COG Long-Term Follow-Up Guidelines.
Vignette. A 2-year-old girl is brought to the emergency department after her caregiver reports she “fell into” the bathtub of hot water. On examination, the child has symmetric, well-demarcated, full-thickness burns to both feet up to the ankle, both buttocks, and the perineum, with sparing of the soles, popliteal fossae, and a central zone on the buttocks. There are no splash marks. The caregiver reports the burn occurred two hours before arrival; arrival was delayed because the caregiver was “looking for transportation.” The burn pattern measures 18% total body surface area (TBSA) by Lund-Browder estimation.
What pattern of injury does this constellation suggest, what specific physical findings support that interpretation, what fluid resuscitation formula and rate apply during the first 24 hours, what is the urine output goal in this child, and what is the next step in disposition beyond burn care?
(Answer at the end of this chapter)
Section 1: Pediatric Burn Epidemiology and TBSA Estimation
Bottom line: pediatric burns are the third leading cause of unintentional childhood death, with approximately 100,000 children seeking burn treatment annually in the United States and mortality now under 3% for hospitalized cases. The peak age is 1 to 5 years; scalds from hot liquids dominate in the under-5 group (60% to 80%), flame burns dominate over age 5, and non-accidental trauma (NAT) accounts for 10% to 20% of pediatric burns. The Lund-Browder chart is the gold standard for pediatric TBSA estimation because the head accounts for 18% in young children versus 9% in adults and each leg accounts for 14% versus 18% in adults. First-degree (superficial) burns are NOT counted in TBSA for fluid resuscitation; only partial-thickness and full-thickness burns are included. The palmar method (the patient’s palm plus fingers equals approximately 1% TBSA) supplements both systems for scattered or small burns.
Burns are a leading cause of injury-related morbidity and mortality in children, with approximately 100,000 children seeking burn treatment annually in the United States. Modern critical care has driven mortality for hospitalized pediatric burns to under 3%, but inhalation injury still drives 40% to 60% of burn deaths. The peak incidence is between ages 1 and 5, when toddlers can reach pots, faucets, and curling irons but cannot yet appreciate temperature. In children under 5, scald burns from hot liquids (bathwater, spilled coffee or tea, cooking water) account for 60% to 80% of injuries; over age 5, flame burns become the dominant mechanism as cooking, matches, and outdoor fires enter the activity profile. Contact burns from irons, stoves, and curling irons sit in third place across all ages. Non-accidental trauma (NAT) accounts for 10% to 20% of pediatric burns, a number large enough that every pediatric burn evaluation must include an explicit screen for abuse.
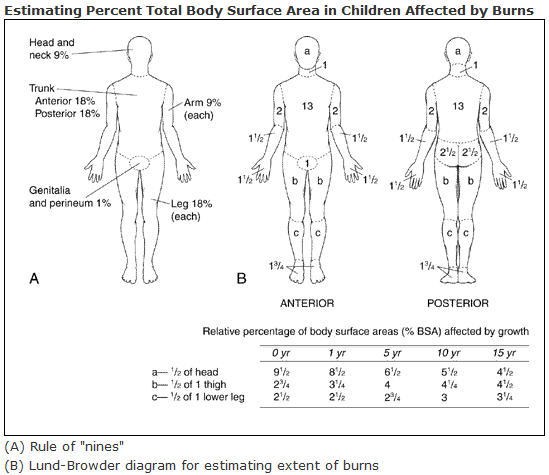
The Wallace rule of nines was designed for adult body proportions and produces systematic overestimates of leg surface area and underestimates of head surface area when applied to children. The modified pediatric rule of nines compensates by reassigning percentages: head and neck 18% (versus 9% in adults), each upper extremity 9% (unchanged), anterior trunk 18% (unchanged), posterior trunk 18% (unchanged), each lower extremity 14% (versus 18% in adults), and perineum/genitalia 1% (unchanged). The pediatric head loses approximately 1% TBSA per year of age from 18% at birth toward 7% in adults, with the legs gaining proportionally. The modified rule of nines is fast at the bedside but still coarse; it works for triage estimation and burn-center referral decisions but should be replaced by the Lund-Browder chart when calculating fluid resuscitation.

Source: Wikimedia Commons contributors, via Wikimedia Commons, CC BY-SA 4.0. https://commons.wikimedia.org/wiki/File:Wallace_rule_of_nines-en.svg The Lund-Browder chart (Lund and Browder, 1944) is the gold standard for pediatric TBSA estimation because it provides explicit age-specific percentages that track the changing proportions of the growing child. Head total runs 19% at 0 to 1 year, 17% at 1 to 4 years, 13% at 5 to 9 years, 11% at 10 to 14 years, and 7% at 15 and older. Each thigh grows from 5.5% in infancy to 9.5% in adulthood, and each lower leg from 5% to 7%. Anterior trunk, posterior trunk, neck, buttocks, genitalia, upper arms, forearms, hands, and feet remain effectively constant across ages. Superficial (first-degree) burns are NOT counted in the TBSA used for fluid resuscitation; only partial-thickness and full-thickness burns are tallied. The palmar method (the patient’s palm including fingers equals approximately 1% TBSA) is useful for estimating scattered or small burns where chart estimation is awkward.
Source: Wikimedia Commons contributor, via Wikimedia Commons, Public Domain Mark 1.0. https://commons.wikimedia.org/wiki/File:Lund-Browder_chart-burn_injury_area.PNG The TBSA estimation has direct downstream consequences. TBSA drives the Parkland fluid volume (covered in Section 2). It drives the ABA burn center referral threshold (partial-thickness burns over 10% TBSA always warrant transfer; full-thickness burns of any size warrant transfer). And it drives the escharotomy decision in circumferential trunk or extremity burns, where a constricting eschar can compromise distal perfusion or chest-wall expansion within hours of injury. Overestimating TBSA by including first-degree burns produces iatrogenic edema from over-resuscitation; underestimating produces under-resuscitation and acute kidney injury. The bedside discipline is to measure carefully, recheck after the initial fluid bolus, and document each estimate.
High Yield — Pediatric TBSA estimation

- Peak age 1 to 5 years. Scalds dominate under 5 (60% to 80%); flame burns dominate over 5.
- NAT accounts for 10% to 20% of pediatric burns. Screen every case.
- Pediatric rule of nines: head 18% (vs adult 9%); each leg 14% (vs adult 18%); arms, trunk, perineum unchanged.
- Lund-Browder head: 19% at 0-1 yr; 17% at 1-4; 13% at 5-9; 11% at 10-14; 7% adult.
- First-degree burns NOT counted in TBSA for fluid resuscitation.
- Palmar method: patient’s palm plus fingers equals approximately 1% TBSA.
- Inhalation injury drives 40% to 60% of burn mortality even when surface area is modest.
Mnemonic — “Head shrinks, legs grow”

As the child ages, the head loses approximately 1% TBSA per year of age (from 18% at birth toward 7% in adults), while each leg gains proportionally (from 14% in young children to 18% in adults). If you can remember the directionality, you can reconstruct any age-band estimate in the moment without memorizing every row.
You are looking at the most excruciatingly painful injury on the chart. But then you see a full-thickness burn where the tissue destruction goes all the way down into the subcutaneous fat, and it’s essentially insensate. Pain is literally inversely correlated with the depth of the burn.
— PEDS-11-a podcast, ~00:30