PEDS · EP 13 · ORTHOTICS
Before You Listen
Episode Setup
- Topic in one line: the pediatric orthotic and assistive technology toolkit, including the supramalleolar orthosis to ground reaction ankle-foot orthosis (GRAFO) selection map, the Winters-Gage-Hicks hemiplegic gait classification, the spina bifida orthotic prescription by neurological level, scoliosis bracing anchored by the BrAIST trial, the early power mobility paradigm shift, augmentative and alternative communication (AAC), the seating hierarchy (“fix the pelvis, free the hands”), and the standardized outcome measures (Gross Motor Function Classification System (GMFCS), Gross Motor Function Measure-66 (GMFM-66), Functional Independence Measure for Children (WeeFIM), Pediatric Evaluation of Disability Inventory (PEDI/PEDI-CAT), Bayley-4, Goal Attainment Scaling (GAS), Canadian Occupational Performance Measure (COPM)) that quantify intervention effect.
- Prerequisites: cerebral palsy GMFCS levels and topographic patterns from PEDS-04, basic gait deviations (equinus, crouch, recurvatum), and the pediatric spasticity management ladder from PEDS-12.
- Runtime: 1 hour 2 minutes.
Vignette. A 6-year-old girl with spastic diplegic cerebral palsy at GMFCS level III is brought to your pediatric rehabilitation clinic for orthotic re-evaluation. Six months ago she received a posterior leaf spring (PLS) ankle-foot orthosis (AFO) bilaterally for what was described as “drop foot.” On observational gait analysis today she walks with a posterior walker, both ankles in approximately 15 degrees of dorsiflexion at midstance, persistent knee flexion of approximately 30 degrees throughout stance, and forward trunk lean. Her quadriceps strength is 4-/5 bilaterally. There is no fixed knee flexion contracture. Her mother reports increased fatigue and frequent falls.
Why is the posterior leaf spring AFO the wrong orthosis for this child, what is the correct orthosis and what is its biomechanical mechanism, what is the contraindication that would block this orthosis if her examination findings were different, what gait pattern in the Winters-Gage-Hicks or diplegic gait classification does she demonstrate, and which standardized outcome measure would best track change in her gross motor function before and after orthotic optimization?
(Answer at the end of this chapter)
Section 1: Pediatric Ankle-Foot Orthoses and Gait Type Matching
Bottom line: the ankle-foot orthosis (AFO) is the most prescribed pediatric lower-extremity orthosis, with usage scaling by GMFCS level (about 30% at level I, 60-70% at level II, more than 80% at level III and above); the supramalleolar orthosis controls the subtalar joint in the coronal plane only, the posterior leaf spring AFO assists swing-phase dorsiflexion for foot drop, the solid AFO blocks all ankle motion for severe equinus or recurvatum, the hinged AFO permits stance-phase dorsiflexion when quadriceps strength is adequate, and the ground reaction AFO is the orthosis for crouch gait.
The ankle-foot orthosis (AFO) is the most commonly prescribed orthosis in pediatric rehabilitation. AFO usage rises with GMFCS level: roughly 30% at GMFCS I, 60-70% at GMFCS II, and over 80% at GMFCS III and above. Each AFO type addresses a specific biomechanical problem and the wrong AFO can worsen gait.
The supramalleolar orthosis (SMO) extends just above the malleoli with trim lines below the malleolar tips. It provides a rigid footplate with medial and lateral walls that encompass the hindfoot and midfoot. The SMO controls hindfoot valgus and varus by stabilizing the subtalar joint in the coronal plane, but it does not control sagittal plane motion at the ankle and permits free dorsiflexion and plantarflexion. The textbook indication is pes planovalgus (pronated foot) and mild hypotonia with foot and ankle instability (commonly seen in Down syndrome). It is inappropriate for any child with equinus, crouch, or any sagittal-plane deviation.
The posterior leaf spring (PLS) AFO consists of a thin posterior strut with inherent flexibility at the ankle and a rigid footplate. The narrow trim lines behind the malleoli allow the strut to flex during push-off. The PLS provides dorsiflexion assistance during swing, preventing foot drop, but allows dorsiflexion and some plantarflexion in stance. It cannot generate a knee extension moment and is therefore inappropriate for crouch gait. The textbook indication is the hemiplegic child with isolated dorsiflexor weakness and adequate quadriceps strength (Winters-Gage-Hicks Type I).
The solid (rigid) AFO has trim lines anterior to the malleoli, blocking all ankle motion. It can be set in neutral or in slight (typically 5 degrees) dorsiflexion. The solid AFO eliminates all sagittal-plane ankle motion, creating a rigid lever during stance. When set in slight dorsiflexion, the solid AFO shifts the ground reaction force vector anteriorly, promoting knee extension. The cost is loss of third rocker (heel rise) and slowed gait velocity. Indications include moderate to severe equinus with poor selective motor control, recurvatum (knee hyperextension) gait, and crouch when quadriceps weakness is severe.
The hinged AFO has a rigid frame with a mechanical hinge at the ankle joint. A plantarflexion stop blocks plantarflexion beyond neutral while permitting dorsiflexion in stance. By allowing third rocker (heel rise), the hinged AFO produces a more normal gait pattern than the solid AFO, but the quadriceps must actively control tibial advancement. The hinged AFO is therefore contraindicated in crouch gait and in children with weak quadriceps, where it will allow collapse into excessive dorsiflexion and worsen the crouch pattern. The textbook indication is dynamic equinus with adequate quadriceps strength (Winters-Gage-Hicks Type II), often after botulinum toxin injection.
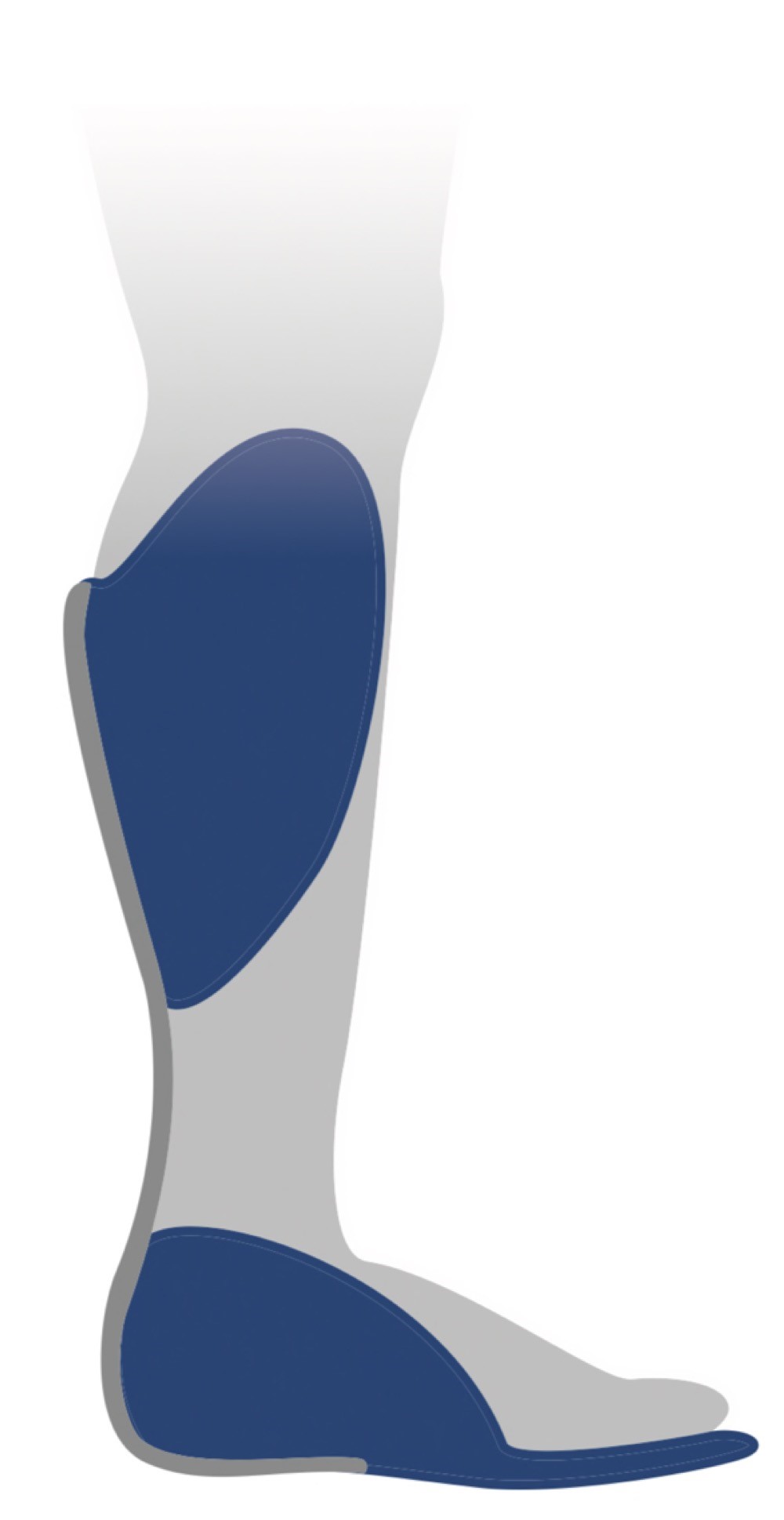
The ground reaction AFO (GRAFO) is a solid AFO set in slight plantarflexion with an anterior tibial shell (clamshell or anterior strap). The anterior shell prevents the tibia from advancing forward over the foot. The GRAFO directs the ground reaction force vector anterior to the knee joint center during stance, generating a passive knee extension moment that compensates for weak quadriceps. The GRAFO is the orthosis for crouch gait. The contraindication is knee flexion contracture exceeding 10-15 degrees (the orthosis cannot generate an extension moment if the knee cannot extend) and equinus gait (wrong biomechanical problem).


Source: Pagemaker787 (Wikimedia Commons), “AFO Ankle Foot Orthosis Orthotic Brace.” CC BY-SA 4.0.
Source: Orthokin (Wikimedia Commons), “Posterior Leaf Spring AFO.” CC BY-SA 4.0.
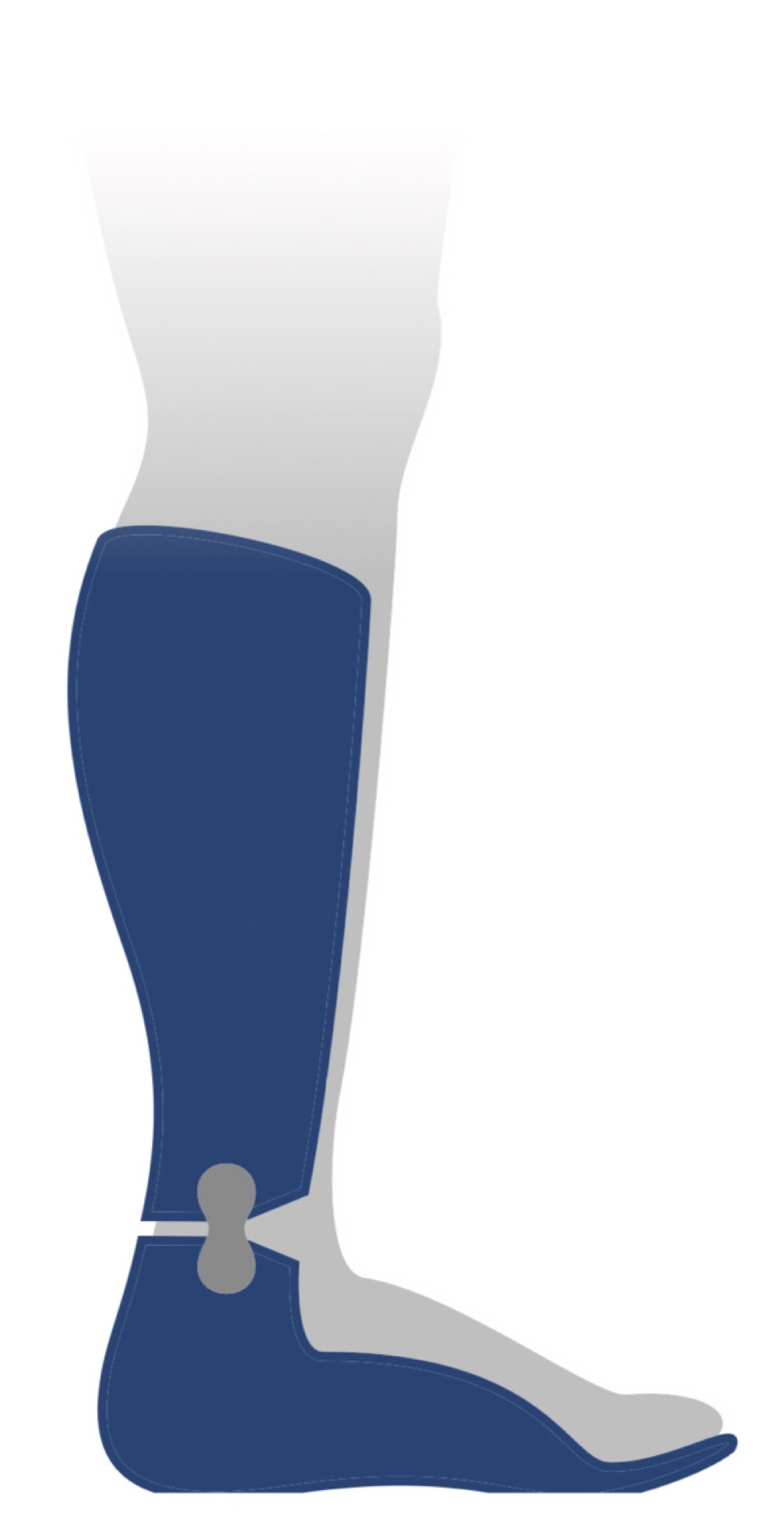
Source: Orthokin (Wikimedia Commons), “Hinged AFO.” CC BY-SA 4.0.
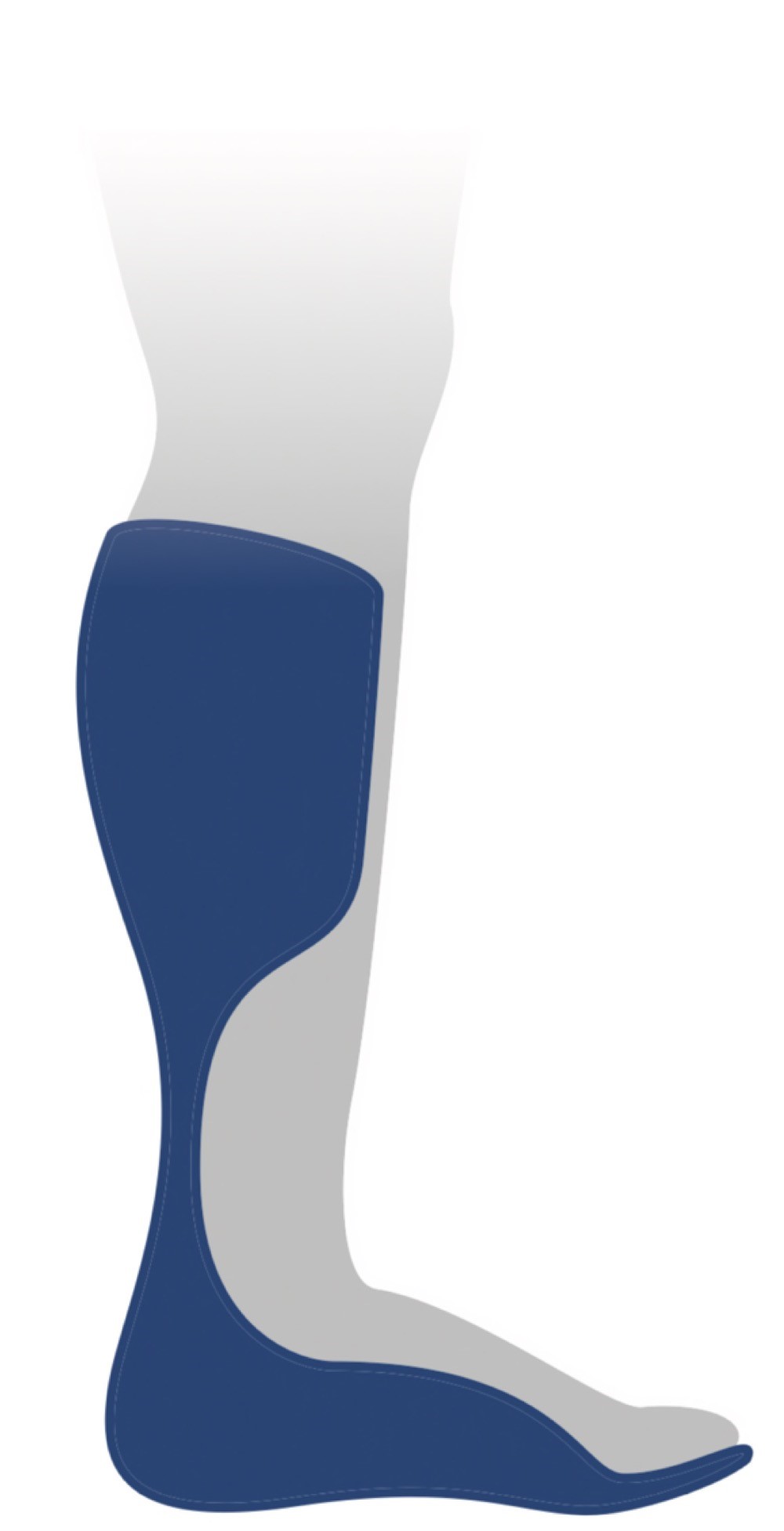
Source: Orthokin (Wikimedia Commons), “DAFO AFO.” CC BY-SA 4.0.
The Winters-Gage-Hicks classification (1987) categorizes hemiplegic gait by sagittal plane involvement. Type I is drop foot in swing only with normal stance, treated with a PLS AFO. Type II is true equinus throughout the gait cycle, treated with a hinged AFO or solid AFO. Type III is equinus plus knee recurvatum or stiff knee, treated with a solid AFO. Type IV is equinus plus knee plus hip plus pelvis involvement, requiring a solid AFO plus consideration of multilevel surgery. Diplegic gait patterns map differently. True equinus (Group 1): PLS or hinged AFO with plantarflexion stop. Jump gait (Group 2) with equinus plus knee and hip flexion: solid or hinged AFO. Apparent equinus (Group 3) where knee flexion creates the appearance of equinus: solid AFO or GRAFO. Crouch gait (Group 4) with excessive dorsiflexion plus persistent knee flexion: GRAFO. Stiff knee gait with reduced swing-phase knee flexion: AFO alone is insufficient and may require botulinum toxin to rectus femoris or distal rectus transfer.
The Owen 2010 framework on AFO tuning integrates the AFO with the shoe to optimize the shank-to-vertical angle during stance. A shank inclined too far forward promotes knee flexion (crouch); a shank too vertical promotes knee hyperextension (recurvatum). Heel height and AFO ankle angle must be calibrated together for the desired knee kinematics.
High Yield — AFO selection by gait type
- SMO = subtalar coronal plane only; pes planovalgus, hypotonia; no sagittal control.
- PLS = swing-phase DF assist; foot drop only; NOT for crouch.
- Solid AFO = blocks all ankle motion; severe equinus, recurvatum.
- Hinged AFO = PF stop, DF allowed in stance; needs adequate quadriceps; not for crouch.
- GRAFO = solid + anterior tibial shell; knee extension moment; the orthosis for crouch; contraindicated by knee flexion contracture greater than 10-15 degrees.
- Winters-Gage-Hicks Type I-IV maps hemiplegic gait to PLS, hinged/solid, solid, solid + multilevel surgery.
Mnemonic — “GRAFO for crouch, NEVER hinged or PLS”

If a board vignette describes a child with spastic diplegia in crouch gait, the answer is GRAFO. The hinged AFO permits dorsiflexion in stance and worsens crouch. The PLS permits dorsiflexion in stance and worsens crouch. Only the GRAFO redirects the ground reaction force vector anterior to the knee and generates the passive knee extension moment that lifts the child out of crouch.
When you put them in a GRAFO, the anterior shell physically blocks the tibia from advancing forward over the foot. By blocking that forward tibial progression, the orthosis directs the ground reaction force vector strongly anterior to the knee joint center. The GRAFO physically forces the knee to straighten during stance, completely compensating for weak quadriceps.
— PEDS-13 podcast, ~14:18