REHAB · EP 07 · PRESSURE
Before You Listen
Episode Setup
- Topic in one line: the National Pressure Injury Advisory Panel (NPIAP) staging system (Stage 1 non-blanchable erythema with intact skin, Stage 2 partial-thickness loss of dermis, Stage 3 full-thickness with visible subcutaneous fat, Stage 4 full-thickness with exposed bone / muscle / tendon, Unstageable obscured by slough or eschar, deep tissue pressure injury / DTPI with persistent purple-maroon discoloration); the most common locations by position (sacrum #1 overall, ischial tuberosities #1 in wheelchair-dependent patients, heel, trochanter, occiput); the biomechanical triad of pressure (capillary closing pressure ~32 mmHg), shear, and friction; the Braden Scale six-subscale risk assessment with thresholds of 18 (at risk), 14 (high risk), and 9 (very high risk); pressure-time prevention (every 2 hours bed turning, every 15 minutes wheelchair weight shifts); cushion and surface selection (foam vs gel vs ROHO air; Group 1 static, Group 2 alternating / low air loss, Group 3 air-fluidized); the five debridement types (sharp, mechanical, autolytic, enzymatic, biologic); dressing selection by exudate; negative pressure wound therapy (NPWT, 75-125 mmHg); osteomyelitis workup (probe-to-bone, MRI, bone biopsy as gold standard, 6 weeks IV antibiotics); Marjolin ulcer; flap selection by location.
- Prerequisites: wound healing physiology (hemostasis, inflammatory, proliferative, remodeling phases) and the basic SCI / immobility framework.
- Runtime: 1 hour 5 minutes.
Vignette. A 32-year-old man with a C5 American Spinal Injury Association Impairment Scale (AIS) A spinal cord injury sustained 6 months ago is admitted to your inpatient rehabilitation unit. He has a wound over the right ischial tuberosity that has been present for 3 months. On examination the wound measures 4 by 5 cm with full-thickness loss, visible subcutaneous fat, no visible bone or tendon, and a yellow fibrinous slough covering approximately 30% of the wound base. There is moderate serous drainage. Surrounding skin is intact without fluctuance or erythema beyond 2 cm from the wound margin. The probe-to-bone test is negative. Braden Scale score is 11. Albumin is 3.0 g/dL; prealbumin is 16 mg/dL. He uses a foam wheelchair cushion and reports performing weight shifts “when he remembers.”
What stage is this pressure injury, what is the most appropriate dressing for the current wound bed, what changes to his wheelchair seating and pressure relief schedule are indicated, and what nutritional and surgical decisions need to be made if the wound fails to progress over the next 4 weeks?
(Answer at the end of this chapter)
Section 1: NPIAP Staging and Common Locations
Bottom line: the National Pressure Injury Advisory Panel (NPIAP) staging system has four numbered stages plus Unstageable and deep tissue pressure injury (DTPI) categories — Stage 1 is intact skin with non-blanchable erythema, Stage 2 is partial-thickness loss of dermis with no granulation/slough/eschar, Stage 3 is full-thickness with visible subcutaneous fat but no bone/tendon/muscle, Stage 4 is full-thickness with exposed bone/tendon/fascia/muscle, Unstageable has slough or eschar obscuring the wound base, DTPI presents as persistent deep red/maroon/purple discoloration of intact skin or blood-filled blister; sacrum is the #1 location overall, ischial tuberosities #1 in wheelchair-dependent patients, occiput is key in children, heels are common in supine bedrest.
The National Pressure Injury Advisory Panel (NPIAP) staging system (formerly NPUAP, renamed 2016) is the universal classification. Six categories: four numbered stages plus Unstageable and deep tissue pressure injury (DTPI).
Stage 1: intact skin with non-blanchable erythema. The skin is not broken. Pressing on the reddened area does not blanch (turn white) and return to red. This non-blanchable quality distinguishes Stage 1 from simple reactive hyperemia (which blanches). In darkly pigmented skin, Stage 1 may not present as visible redness but as a difference in skin temperature, firmness, or moisture. The skin is intact; if broken in any way, it is not Stage 1.
Stage 2: partial-thickness loss of skin with exposed dermis. Wound bed is pink or red, moist, and may present as an intact or ruptured serum-filled blister or a shallow open ulcer. The critical distinction is what you do not see: Stage 2 has no granulation, slough, or eschar. If any of these are present, the wound is deeper than Stage 2. Stage 2 does not extend into the subcutaneous fat (only epidermis and dermis are involved).
Stage 3: full-thickness skin loss. Subcutaneous fat is visible in the wound bed, and undermining and tunneling may be present. Bone, tendon, and muscle are not visible or directly palpable; if they are, the wound is Stage 4. Slough and eschar may be present but do not obscure the depth determination. Stage 3 depth varies by location: over the bridge of the nose, ear, or occiput where subcutaneous tissue is thin, Stage 3 is shallow; over the sacrum or buttock, Stage 3 may be very deep.
Stage 4: full-thickness skin and tissue loss with exposed or directly palpable bone, tendon, fascia, or muscle. The most severe staged category, with slough, eschar, undermining, and tunneling common. Osteomyelitis and sepsis are significant risks.
Unstageable: wound bed obscured by slough (yellow, tan, gray, green, or brown) or eschar (tan, brown, or black adherent tissue). The true depth and stage cannot be determined until the slough or eschar is removed by debridement. Once debrided, the wound is staged by the deepest tissue visible. Important exception: stable, dry, adherent eschar on the heel should NOT be removed because it serves as a natural biologic cover for the underlying tissue. Leave it intact and monitor; if it becomes fluctuant, boggy, draining, or develops signs of infection, debride.
Deep tissue pressure injury (DTPI): persistent deep red, maroon, or purple discoloration of intact skin or a blood-filled blister. Discoloration does not blanch and may be preceded by pain, firmness, bogginess, or temperature changes. DTPI represents damage to deep tissues at the bone-muscle interface; injury originates from the inside out and may evolve rapidly into a full-thickness wound over days to weeks. Surface appearance initially underrepresents the severity of underlying injury.

Source: Nanoxyde, Wikimedia Commons, CC BY-SA 3.0
Source: S.raeder, Wikimedia Commons, CC0 1.0 Public Domain
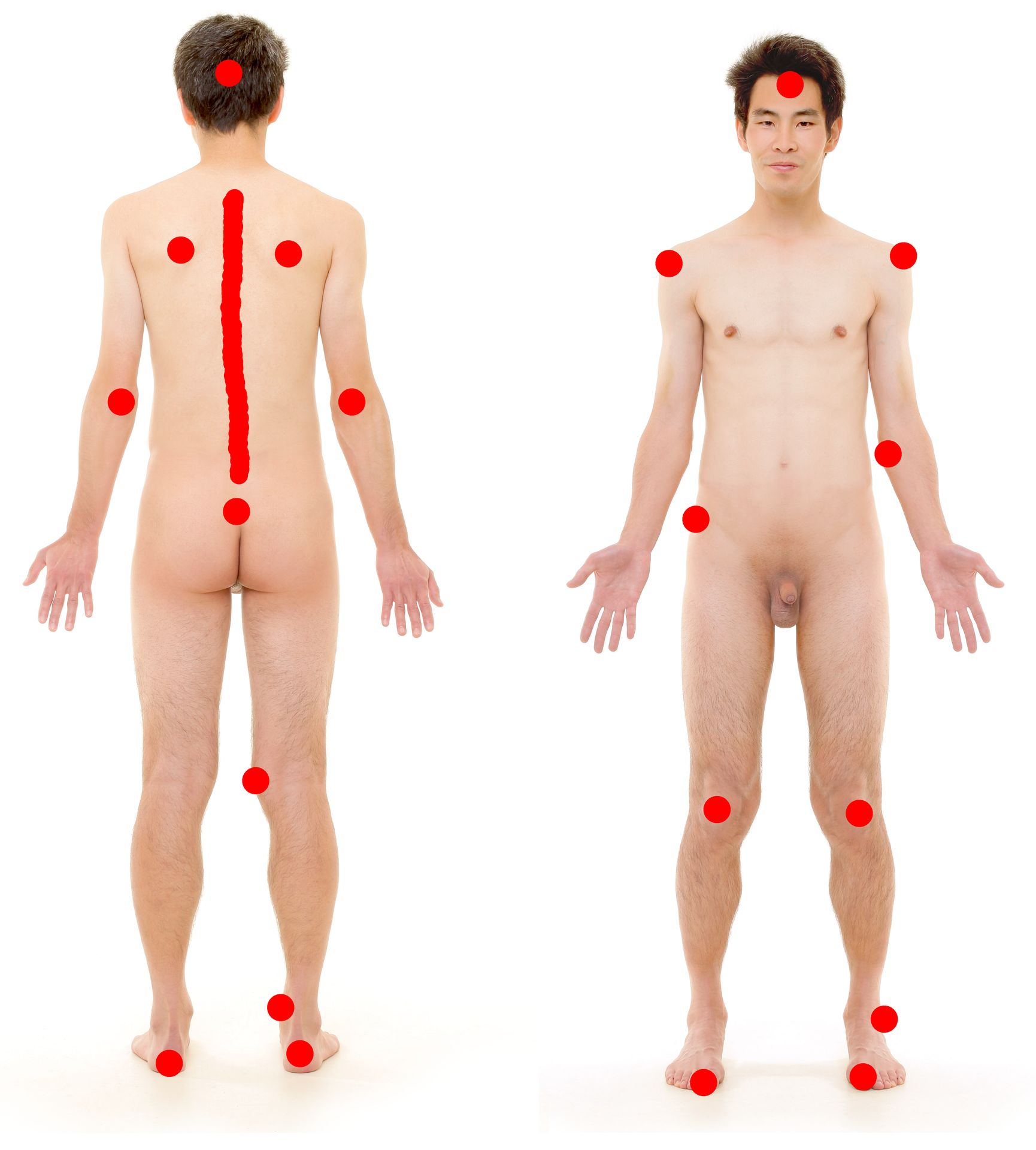
Locations by position are heavily tested. Supine: sacrum is the #1 location overall. Other supine sites: occiput (key in children whose heads are proportionally larger), scapulae, elbows, heels. Side-lying: greater trochanter (primary), lateral malleolus, lateral knee, lateral ribs, ear. Seated: ischial tuberosities are #1 in wheelchair-dependent patients (including SCI). Body weight concentrates over two small bony prominences, generating the highest interface pressures. Sacrum and scapulae are also at risk in seated postures.
High Yield — NPIAP staging and locations
- Stage 1: intact skin, non-blanchable erythema.
- Stage 2: partial-thickness, exposed dermis, blister or shallow ulcer, no granulation/slough/eschar.
- Stage 3: full-thickness, visible subcutaneous fat, no bone/tendon/muscle.
- Stage 4: full-thickness, visible bone/tendon/fascia/muscle.
- Unstageable: slough or eschar obscures base. Heel eschar exception: leave dry stable eschar in place.
- DTPI: persistent purple-maroon intact skin or blood-filled blister; injury from the inside out.
- Sacrum = #1 overall; ischial tuberosities = #1 in wheelchair users; occiput key in children.
Mnemonic — “Skin, Dermis, Fat, Bone”
The four numbered NPIAP stages map to the deepest tissue visible: Stage 1 intact Skin; Stage 2 exposed Dermis; Stage 3 visible Fat (subcutaneous); Stage 4 exposed Bone (or tendon, fascia, muscle). When you see slough or eschar that obscures depth, the wound is Unstageable until debrided.