Chronic Pelvic Pain and Sexuality
REHAB · EP 14 · PELVIS
Before You Listen
- Prerequisites: pelvic floor anatomy (levator ani group, obturator internus, coccygeus), the autonomic axis (parasympathetic S2-S4 and sympathetic T11-L2), the upper motor neuron versus lower motor neuron distinction relevant to spinal cord injury (SCI), and the energy crisis hypothesis of myofascial pain from REHAB-02.
- Runtime: 1 hour 10 minutes.
- Topic in one line: the multidisciplinary approach to chronic pelvic pain (defined as pain perceived in pelvic structures lasting at least 6 months) including pelvic floor dysfunction (hypertonic / non-relaxing levator ani), specific syndromes (vulvodynia, coccygodynia, levator ani syndrome, pudendal neuralgia and the Nantes criteria, interstitial cystitis or bladder pain syndrome, endometriosis, irritable bowel syndrome [IBS]); the physiology of sexual function (parasympathetic for erection or arousal, sympathetic for ejaculation or orgasm); the spinal cord injury (SCI) framework “point and shoot” (S2-S4 reflexogenic erection plus T11-L2 psychogenic erection); pharmacologic and procedural treatment of erectile dysfunction (phosphodiesterase type 5 [PDE5] inhibitors, vacuum erection devices, intracavernosal alprostadil, penile prosthesis); fertility (penile vibratory stimulation [PVS], electroejaculation, autonomic dysreflexia [AD] precaution at T6 and above); sexuality after stroke, traumatic brain injury (TBI), and multiple sclerosis (MS); the metabolic-equivalent (MET) requirement for sex after myocardial infarction (MI) or congestive heart failure (CHF); the Permission, Limited Information, Specific Suggestions, Intensive Therapy (PLISSIT) counseling model; and interventional procedures (pelvic floor botulinum toxin [BoNT], ganglion impar block, superior hypogastric plexus block).
Vignette. A 32-year-old woman presents with 14 months of deep pelvic pain, dyspareunia, urinary frequency without infection, and constipation. On internal examination by a pelvic floor physical therapist, the levator ani and obturator internus are tender with palpable taut bands, and resting electromyographic (EMG) activity is elevated. Three months earlier, an outside provider prescribed Kegel exercises and her pain has worsened.
What is the diagnosis, why did Kegel exercises worsen the pain, what is the first-line treatment, what additional differential should be entertained, and what is the appropriate counseling framework if she also reports avoiding intimacy with her partner?
(Answer at the end of this chapter)
Section 1 — Pelvic Floor Dysfunction and Specific Pelvic Pain Syndromes
Bottom line: chronic pelvic pain affects approximately 15% of women and requires a multidisciplinary approach; pelvic floor dysfunction is the musculoskeletal cornerstone, with hypertonic (non-relaxing) levator ani driving most cases through an energy-crisis mechanism identical to myofascial pain elsewhere; the specific syndromes are vulvodynia, coccygodynia, levator ani syndrome, and pudendal neuralgia; pelvic floor physical therapy is first-line and Kegel exercises are contraindicated in hypertonic dysfunction.
Chronic pelvic pain is persistent or recurrent pain perceived in pelvic structures, lasting at least 6 months. It affects approximately 15% of women and is frequently underdiagnosed. Men are also affected (chronic prostatitis / chronic pelvic pain syndrome [CP/CPPS], NIH category III). The diagnostic challenge stems from convergence of multiple organ systems in the pelvis: musculoskeletal, gynecologic, urologic, gastrointestinal, and neurologic. The board examination tests pelvic pain from a physiatric perspective, emphasizing musculoskeletal and neurologic contributors. The central sensitization model applies: visceral pain from one organ can trigger pelvic floor hypertonicity and myofascial pain, which amplifies the original visceral pain in a self-perpetuating cycle requiring multidisciplinary intervention.
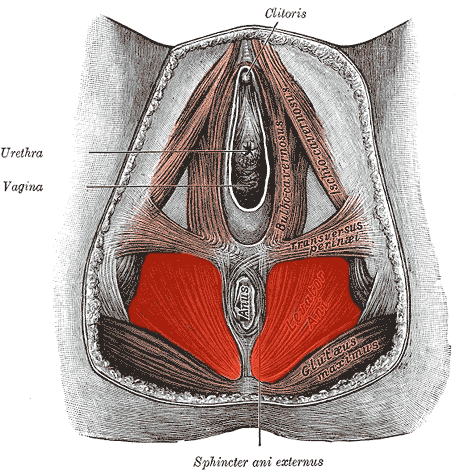
Pelvic floor dysfunction is the musculoskeletal cornerstone. The pelvic floor is a muscular hammock composed of the levator ani group (pubococcygeus, puborectalis, iliococcygeus), the coccygeus, and the obturator internus (functionally integrated with the pelvic floor). These muscles support the pelvic organs, maintain continence, and contribute to sexual function.
Hypertonic pelvic floor dysfunction (non-relaxing pelvic floor) is the pattern most commonly associated with chronic pelvic pain: muscles are in chronic contraction, unable to fully relax. Sustained contraction causes ischemia, metabolic waste accumulation, trigger point formation, and pain. This is the energy crisis hypothesis (REHAB-02) applied to the pelvic floor: sustained contraction compresses capillaries, depletes ATP, and prevents calcium reuptake into the sarcoplasmic reticulum, perpetuating contraction. Patients report deep pelvic pain, pain with sitting, dyspareunia, urinary frequency and urgency without infection, hesitancy, and constipation or painful defecation.
Source: Levator ani and coccygeus, superior view. After Gray’s Anatomy (1918), modified by Uwe Gille, Wikimedia Commons (Public Domain). https://commons.wikimedia.org/wiki/File:Levator_ani.png
On examination, internal digital examination by a trained examiner palpates the levator ani and obturator internus assessing tenderness, trigger points, taut bands, and ability to voluntarily contract and relax the pelvic floor. Many patients with hypertonic pelvic floor cannot relax on command. This inability to downtrain is the hallmark finding.
Pelvic floor electromyography (EMG) is diagnostic and therapeutic. Surface EMG sensors placed intravaginally or intrarectally measure electrical activity in real time. In hypertonic dysfunction, baseline resting EMG is elevated and the patient cannot achieve full relaxation on volitional downtrain commands; the resting baseline never returns to normal. EMG also drives biofeedback therapy: the patient watches the signal and practices reducing the amplitude.
Treatment centers on pelvic floor physical therapy as first-line: internal and external manual therapy with trigger point release of the levator ani, obturator internus, and piriformis; sustained pressure until the taut band releases; and myofascial release of connective tissue restrictions.
Biofeedback using surface EMG trains relaxation of the chronically contracted muscles, the therapeutic reverse of Kegel exercises (which train contraction for stress urinary incontinence). Prescribing Kegels in hypertonic pelvic floor dysfunction worsens the problem by strengthening already over-contracted muscles.
Pharmacologic adjuncts: muscle relaxants (cyclobenzaprine), diazepam suppositories (intravaginal for localized relaxation), neuropathic agents (gabapentin, amitriptyline) for central sensitization, and trigger point injections (local anesthetic alone or with botulinum toxin [BoNT] for refractory levator ani / obturator internus trigger points).
Specific pelvic pain syndromes add to the differential. Vulvodynia is chronic vulvar pain at least 3 months without identifiable cause (no infection, dermatologic condition, or malignancy). It may be localized (vestibulodynia, provoked at the vulvar vestibule with touch) or generalized. The cotton swab test maps reproducible burning or sharp pain at vestibular points. Treatment: topical lidocaine before intercourse, pelvic floor PT for secondary hypertonicity, neuropathic agents (gabapentin, amitriptyline), and cognitive behavioral therapy.
Coccygodynia is coccyx pain worsened by sitting and sit-to-stand transition. Causes: direct trauma (fall onto tailbone), repetitive microtrauma, coccygeal hypermobility, postpartum injury. Dynamic lateral radiographs in seated and standing positions demonstrate hypermobility (more than 20 degrees of flexion). Treatment: donut or wedge cushion (offloads to ischial tuberosities), manual therapy with intrarectal manipulation, pelvic floor PT, local corticosteroid at the sacrococcygeal junction, and coccygectomy for refractory cases.
Levator ani syndrome is chronic anorectal pain from levator spasm: dull rectal ache, worse with sitting, often left-sided. On digital rectal exam, the levator is tender and taut and palpation reproduces the pain. It differs from proctalgia fugax (sudden fleeting rectal pain lasting seconds to minutes, not provoked by exam, internal anal sphincter spasm). Treatment: pelvic floor PT with biofeedback, sitz baths, electrogalvanic stimulation.
Pudendal neuralgia is neuropathic pain from irritation or compression of the pudendal nerve. The nerve arises from S2-S4, exits through the greater sciatic foramen, courses around the ischial spine and sacrospinous ligament, and re-enters through the lesser sciatic foramen to traverse the pudendal canal (Alcock canal) on the medial wall of the ischial tuberosity within obturator internus fascia. Compression points: between sacrospinous and sacrotuberous ligaments, and within Alcock canal.
The classic presentation is burning, aching, or electric perineal pain in the pudendal distribution (perineum, vulva or scrotum, perianal region). Hallmark: pain worsens with sitting and improves with standing or on a toilet seat (which removes Alcock canal pressure). Informally called “cyclist syndrome” from narrow-seat compression.
The Nantes criteria require all five: pain in pudendal territory, predominantly while sitting, no nocturnal awakening, no objective sensory loss, and relief with a diagnostic pudendal nerve block. The block is performed under fluoroscopy or CT at the ischial spine. Treatment: avoidance of provocative positions, cutout cushion, pelvic floor PT, neuropathic agents (gabapentin, pregabalin, tricyclics), repeat blocks, and surgical decompression for refractory cases.

Source: Pudendal nerve, course and branches. Mikael Häggström, Wikimedia Commons (Public Domain). https://commons.wikimedia.org/wiki/File:REHAB-14-02-pudendal-nerve-nantes.svg
Other pelvic nerve entrapments complete the differential. Iliohypogastric (T12, L1): suprapubic pain from internal oblique entrapment or scar from lower abdominal incisions (cesarean sections). Ilioinguinal (L1): runs parallel and inferior; same surgical entrapment produces inguinal and medial thigh pain. Genitofemoral (L1-L2): groin and medial proximal thigh pain. A common board scenario: chronic groin pain after inguinal hernia repair, sharp burning radiating to medial thigh and labia or scrotum, worse with hip extension — answer is ilioinguinal nerve entrapment; next step is a nerve block.
Endometriosis, interstitial cystitis, and IBS frequently overlap. Endometriosis (endometrial tissue outside the uterine cavity) causes cyclical inflammation, adhesions, and pain. Interstitial cystitis (bladder pain syndrome) is pelvic pain related to the bladder with urgency and frequency; pain worsens with bladder filling and is relieved after voiding (diagnostic fill-empty pattern). Cystoscopy may reveal glomerulations or Hunner ulcers. The potassium sensitivity test instills potassium chloride; greater pain than saline indicates epithelial permeability (damaged glycosaminoglycan layer). IBS uses the Rome criteria (recurrent abdominal pain at least one day per week for 3 months, associated with defecation and stool changes). These three overlap through visceral cross-sensitization (shared spinal segments, convergent afferents), reinforcing the multidisciplinary approach.

Board Trap — “Kegels for chronic pelvic pain”
Wrong direction. Prescribing Kegel exercises in hypertonic pelvic floor dysfunction worsens the problem because it strengthens muscles already in excessive contraction. The deficit is the inability to relax, not the inability to contract. Pelvic floor physical therapy with biofeedback for downtraining is first-line; Kegels are reserved for hypotonic conditions like stress urinary incontinence.
High Yield: Pelvic floor and pelvic pain syndromes
- Chronic pelvic pain affects approximately 15% of women; multidisciplinary approach.
- Hypertonic pelvic floor dysfunction is the most common contributor; energy crisis hypothesis applied to the pelvic floor.
- Pelvic floor physical therapy is first-line; biofeedback EMG for downtraining; NOT Kegels.
- Vulvodynia: cotton swab test; topical lidocaine, gabapentin, amitriptyline.
- Coccygodynia: dynamic radiographs (over 20 degrees flexion = hypermobility); donut cushion.
- Levator ani syndrome vs proctalgia fugax (smooth muscle, brief episodes).
- Pudendal neuralgia: pain worse sitting, better on toilet seat; Nantes criteria; block at ischial spine.
- Ilioinguinal nerve entrapment after hernia repair: sharp groin pain radiating to medial thigh.
- Interstitial cystitis: pain worse with bladder filling, relieved after voiding; glomerulations, Hunner ulcers.
So if you tell that patient to go home and do three sets of 10 Kegel exercises every day, you’re demanding that an already hypoxic locked muscle contract even harder. You are actively worsening the ischemia. The muscle does not need to be strengthened. It desperately needs to be released.
— REHAB-14 podcast, ~06:03