Autonomic Dysreflexia
SCI · EP 05 · NEUROTRAUMA
Before You Listen
- Prerequisites: ASIA Impairment Scale (AIS) classification and the meaning of complete (AIS A) versus incomplete (AIS B/C/D) injuries; the splanchnic sympathetic outflow from T5–L2 and the intermediolateral cell column; the resolution of spinal shock and the return of segmental reflexes; baseline autonomic findings in cervical spinal cord injury (SCI), including resting hypotension.
- Runtime: 1 hour 21 minutes.
- Topic in one line: the T6 splanchnic threshold, the 20 mmHg systolic blood pressure (SBP) rule above a low SCI baseline, the bladder-bowel-skin trigger search order with the 85% bladder-first weight, the seven-step management algorithm starting with sit-up and ending with topical 2% nitroglycerin paste, the absolute phosphodiesterase-5 inhibitor (PDE5) contraindication, the pure beta-blocker contraindication, the labor-versus-preeclampsia distinction in pregnant SCI patients, silent autonomic dysreflexia (AD), and the boosting prohibition under the International Paralympic Committee (IPC).
Vignette. A 26-year-old man with a complete C5 AIS A tetraplegia, 8 months post-injury, develops a sudden pounding bifrontal headache, profuse sweating across his face and neck, and goosebumps over his thighs while watching television. His baseline SBP is 92 mmHg. The bedside cuff reads 168/104 mmHg with a heart rate of 112 bpm. His indwelling Foley appears clamped against the bedrail. His wife mentions he took sildenafil approximately 6 hours earlier.
What is the diagnosis, the immediate non-pharmacologic intervention, the first organ system to investigate, and which first-line antihypertensive agent is absolutely contraindicated?
Section 1: Splanchnic Anatomy and the T6 Threshold
Bottom line: autonomic dysreflexia (AD) requires a complete enough lesion at T6 or above to disconnect the entire splanchnic sympathetic outflow (T5–L2) from supraspinal inhibition; the splanchnic vascular bed receives about 25% of cardiac output, so its unopposed vasoconstriction below the lesion drives the hypertensive crisis above it.
In the intact nervous system, sympathetic preganglionic neurons live in the intermediolateral cell column (IML), a vertical strip of gray matter spanning T1 through L2. These neurons control vascular tone in the trunk, abdomen, and lower extremities, and they are under continuous inhibition from the brainstem. Descending fibers from the rostral ventrolateral medulla, the nucleus tractus solitarius, and the hypothalamus travel through the lateral funiculus and act as a tonic brake on sympathetic output. When a noxious stimulus arises below a given segment, afferent signals ascend; the brain evaluates the stimulus, decides whether the response should be reflexive or trivial, and modulates the sympathetic outflow through those same descending pathways. Routine afferent traffic from a stretching bladder or a tight sock never reaches a vascular response in the able-bodied person because the supraspinal brake adjusts the local reflex amplitude in real time.
Spinal cord injury (SCI) at or above T6 physically transects the descending inhibitory pathways. The reflex arc below the lesion remains intact, but the brake is gone. A noxious stimulus below the lesion activates afferent fibers, which enter the cord and excite sympathetic preganglionic neurons in the IML. Without the descending sympatholytic signal, the response is unopposed, uninhibited, and amplified. The result is widespread vasoconstriction in the splanchnic, renal, and lower-extremity vascular beds. The splanchnic bed alone normally receives approximately 25% of cardiac output, so its sudden constriction translates to a dramatic systemic blood pressure surge. Carotid and aortic baroreceptors detect the rise and trigger compensatory parasympathetic outflow through the vagus nerve: the heart slows at the sinoatrial node, and vessels above the lesion dilate. Those compensations cannot reach the constricted territory below the lesion because the sympatholytic signal cannot cross the spinal lesion. The trigger keeps firing, the brake stays disconnected, and pressure stays dangerously elevated until the stimulus is removed or pharmacologically suppressed.
The T6 threshold is anatomic, not arbitrary. The greater splanchnic nerve arises from T5–T9, the lesser splanchnic from T10–T11, and the least splanchnic from T12. Together they innervate the celiac, superior mesenteric, and inferior mesenteric ganglia, which control the splanchnic vascular bed. Lesions at T6 or above disconnect the entire splanchnic sympathetic outflow from supraspinal control, exposing the largest rapidly mobilizable vascular reservoir to unopposed reflex activation. Lesions below T6 leave enough supraspinal influence over splanchnic tone that severe AD does not occur. Cases at T7 or T8 are reported in some series, but T6 is the threshold the boards use, and the splanchnic-bed argument is the answer to the “why T6?” stem.
Severity also tracks completeness. A patient with a complete C5 AIS A injury will have more frequent and more severe episodes than a patient with an incomplete C5 AIS C injury, because incomplete lesions preserve some descending inhibitory fibers that partially suppress the reflex. The board framing is “which patient is at highest risk for severe AD?” The answer is the patient with the highest and most complete injury. AD affects 48–90% of patients with susceptible injuries and develops after spinal shock has resolved. Onset typically falls between 2 and 4 weeks and 2 months post-injury, coinciding with the return of segmental reflexes. Cases as early as 4 days have been documented. Greater than 90% of susceptible patients experience their first episode within the first year, and episodes tend to become more frequent and more predictable as the spinal reflex circuitry potentiates over time.

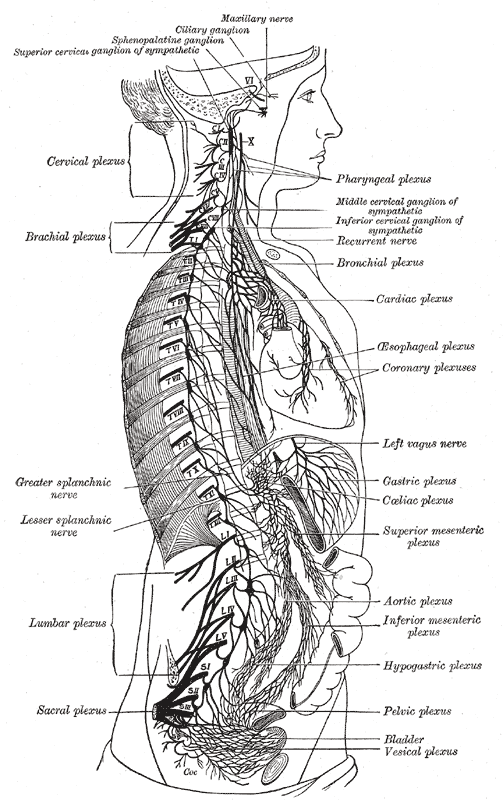
Source: Wikimedia Commons / Gray’s Anatomy plate 848 (Public Domain).
High Yield — Why T6

- T6 is the threshold because of splanchnic anatomy. The greater (T5–T9), lesser (T10–T11), and least (T12) splanchnic nerves drive a vascular bed that holds ~25% of cardiac output. Lesions at T6 or above disconnect the entire outflow.
- AD requires the loss of supraspinal sympatholytic control. The reflex arc below the lesion is intact; the brake from the rostral ventrolateral medulla, the nucleus tractus solitarius, and the hypothalamus is gone.
- Completeness matters. Complete (AIS A) injuries produce more frequent and more severe episodes than incomplete (AIS B/C/D) injuries at the same level.
- Onset is post-spinal shock. Most first episodes occur 2–4 weeks to 2 months post-injury; >90% within the first year.
- Prevalence is 48–90% of patients with injuries at T6 or above.
Board Trap — “Below T6 can’t be AD”

The classic teaching is “T6 and above,” but isolated cases at T7 or T8 are reported in the literature. The board answer is still T6 or above because that is the anatomic threshold tied to the splanchnic outflow. If a stem describes a clean AD picture in a T8 patient with hypertension and a pounding headache during catheterization, the diagnosis remains AD. The splanchnic argument is the right reason; “T6 by tradition” is not.
It’s the largest rapidly mobilizable reservoir of blood in the human body.
— SCI-05 podcast, ~00:57