Neurogenic Bladder Management
SCI · EP 06 · UROLOGY
Before You Listen
- Prerequisites: spinal cord injury (SCI) anatomy from T11–L2 (sympathetic) and S2–S4 (parasympathetic and somatic); the difference between upper motor neuron (UMN) and lower motor neuron (LMN) lesions; ASIA Impairment Scale (AIS) classification; the autonomic dysreflexia (AD) trigger framework from SCI-05.
- Runtime: 1 hour 24 minutes.
- Topic in one line: the priority hierarchy with renal preservation first; sympathetics-store / parasympathetics-pee receptor wiring (alpha-1 outlet, beta-3 detrusor, M3 detrusor, nicotinic external sphincter); UMN versus LMN bladder patterns and detrusor-sphincter dyssynergia (DSD); the spinal-shock to clean intermittent catheterization (CIC) transition; the McGuire 40 cmH2O detrusor leak point pressure (DLPP) threshold; oxybutynin versus trospium; mirabegron and intradetrusor onabotulinumtoxinA at 200 units; the asymptomatic bacteriuria rule; and the catheter-associated squamous-cell bladder cancer risk after >10 years.
Vanilloid receptor agonists (capsaicin and resiniferatoxin) are an investigational class targeting the TRPV1 (transient receptor potential vanilloid 1) receptor on C-fiber afferents. In normal bladders, sensation is carried predominantly by myelinated A-delta fibers; after SCI, C-fiber afferents sprout and become the dominant hyperactive sensory pathway driving reflex detrusor overactivity. Intravesical capsaicin (and the more potent ultrapotent agonist resiniferatoxin / RTX, derived from Euphorbia resinifera) initially excites then desensitizes TRPV1-expressing C-fibers, producing weeks-to-months of detrusor overactivity reduction. Capsaicin causes an immediate burning sensation requiring intravesical anesthesia; RTX is paradoxically less acutely irritating. Neither has FDA approval for neurogenic detrusor overactivity; they are used investigationally or off-label in refractory disease.
Vignette. A 31-year-old woman with a complete T6 AIS A paraplegia, 18 months post-injury, manages her bladder with clean intermittent catheterization (CIC) every 6 hours and oxybutynin 5 mg orally three times daily. She reports increasing urgency between catheterizations, two breakthrough leaks per day, and one episode of pounding headache and facial sweating during a recent catheterization. Urodynamics show involuntary detrusor contractions starting at 180 mL with electromyographic activity in the external sphincter during contraction; the DLPP is 48 cmH2O, and post-void residual volume after CIC is 30 mL. She also reports persistent dry mouth and “feeling foggy” since starting oxybutynin.
What is the urodynamic diagnosis, what is the safety threshold this DLPP has crossed, what pharmacologic switch best addresses both the cognitive side effects and the failure to control storage, and what is the next-line therapy if oral medications do not normalize the DLPP?
Section 1: Wiring of Micturition and the Priority Hierarchy
Bottom line: bladder management in SCI exists to preserve the upper urinary tract (the kidneys), with continence and convenience ranking below renal protection; voiding requires the cortex, the pontine micturition center, and the sacral reflex arc, and the level of disconnection determines the dysfunction pattern.
Neurogenic bladder dysfunction affects virtually every patient with a clinically significant spinal cord injury (SCI) and remains one of the most consequential long-term complications. Before the modern era of clean intermittent catheterization (CIC) and urodynamic surveillance, renal failure was the leading cause of death in persons with SCI. That outcome has changed dramatically, but urologic complications remain a principal source of morbidity, rehospitalization, and diminished quality of life in this population.
The priority hierarchy is fixed and tested. First and above all else: preservation of the upper urinary tract (the kidneys). Second: prevention of urinary tract infection (UTI). Third: efficient bladder emptying. Fourth: avoidance of indwelling catheterization when possible. Fifth: patient concordance with the management plan. Sixth: minimization of pharmacologic burden when feasible. The teaching point is that renal preservation outranks continence and convenience. A patient who is dry but developing silent kidney damage from unchecked intravesical pressure is being managed incorrectly. A patient who has occasional leaks but maintains a safe, low-pressure storage profile is being managed correctly.
Normal micturition requires coordinated interaction between cortical, brainstem, and spinal centers, and the boards test each level because lesions at different levels produce different dysfunction patterns. The cerebral cortex, specifically the medial prefrontal cortex and anterior cingulate gyrus, exerts tonic inhibition over the sacral micturition center during the storage phase. When this cortical inhibition is damaged (stroke, tumor, traumatic brain injury), the patient develops detrusor overactivity with preserved sphincter coordination. The clinical picture is urgency and urge incontinence without detrusor-sphincter dyssynergia (DSD). The pontine micturition center, also known as Barrington nucleus, is the master switch that coordinates voiding. When the cortex releases its inhibitory hold, the pontine micturition center simultaneously activates parasympathetic efferents to contract the detrusor and inhibits the external urethral sphincter via the pudendal nucleus (Onuf nucleus) in the sacral cord. This reciprocal coordination ensures detrusor contraction and sphincter relaxation occur together. The sacral micturition center resides in the intermediolateral cell column at S2–S4 and contains the parasympathetic preganglionic neurons that drive detrusor contraction; Onuf nucleus, in the ventral horn at the same levels, contains the somatic motor neurons innervating the external urethral sphincter via the pudendal nerve.
Lesions disconnect different levels of this circuit. Suprapontine lesions (above the pons) leave the pontine coordination intact, so detrusor and sphincter remain synchronized; the patient gets urgency and urge incontinence without DSD. Suprasacral lesions below the pons (the typical SCI pattern from cervical or thoracic injuries) disconnect the pontine micturition center from the sacral center; reflex detrusor contractions still occur because the sacral arc is intact, but the sphincter contracts simultaneously instead of relaxing, producing DSD with dangerously elevated intravesical pressures. Sacral or cauda equina lesions destroy the parasympathetic preganglionic neurons and the reflex arc itself; the bladder becomes areflexic with overflow incontinence at large volumes.

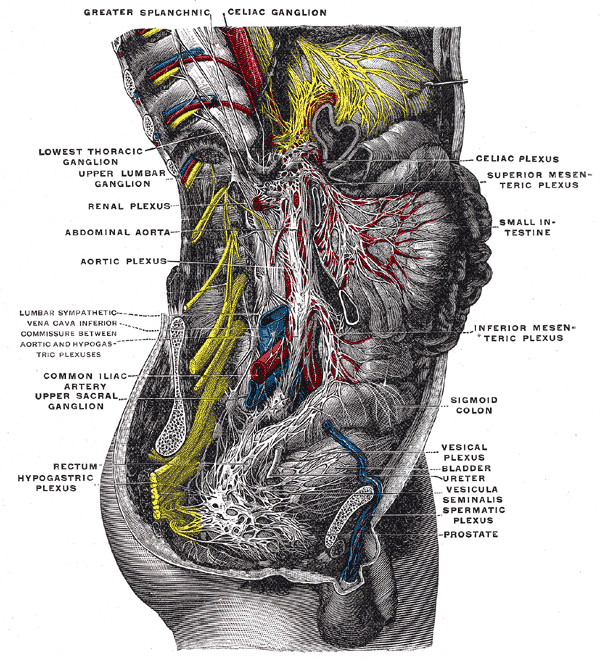
Source: Henry Gray, Anatomy of the Human Body (1918), Plate 849 via Wikimedia Commons (public domain).
Three peripheral nerve systems control the lower urinary tract, and the boards expect all three cold. The mnemonic is sympathetics store, parasympathetics pee. Parasympathetic innervation arises from S2–S4 via the pelvic nerve; postganglionic acetylcholine acts on M3 muscarinic receptors on detrusor smooth muscle to produce contraction (voiding). Sympathetic innervation arises from T11–L2 via the hypogastric nerve and exerts a dual storage function: alpha-1 adrenergic receptors at the bladder neck and internal urethral sphincter mediate smooth muscle contraction (outlet tightening), and beta-3 adrenergic receptors on the detrusor body mediate smooth muscle relaxation (bladder accommodation during filling). Somatic innervation arises from S2–S4 via the pudendal nerve and carries motor fibers from Onuf nucleus to the external urethral sphincter (striated skeletal muscle under voluntary control via nicotinic cholinergic receptors). The receptor pharmacology directly maps to drug mechanisms in Section 4.
High Yield — Wiring and priorities

- Renal preservation is priority 1. Continence and convenience rank below kidney protection.
- Three centers control micturition: cortex (storage inhibition), pontine micturition center (coordination), sacral S2–S4 (reflex arc).
- Suprapontine lesion = overactive bladder, no DSD. Suprasacral SCI = DSD with hostile high-pressure bladder. Sacral/cauda equina = areflexia and overflow.
- Sympathetics store, parasympathetics pee. Sympathetic = T11–L2 hypogastric, alpha-1 outlet contraction + beta-3 detrusor relaxation. Parasympathetic = S2–S4 pelvic, M3 detrusor contraction. Somatic = S2–S4 pudendal, nicotinic external sphincter.
- Renal failure was historically the leading cause of death in SCI before CIC and urodynamic surveillance changed practice.
If you are looking at a patient’s chart and they are perfectly dry, meaning they never leak a drop of urine, but they have a high pressure bladder that is silently blasting urine back up into their kidneys, that patient is being managed incorrectly. They are a ticking time bomb.
— SCI-06 podcast, ~02:46