Neurogenic Bowel and GI Complications
SCI · EP 07 · NEUROGENICBOWEL
Before You Listen
- Prerequisites: spinal cord neuroanatomy from SCI-01 (conus medullaris, cauda equina, sacral reflex arc); basic autonomic nervous system organization (sympathetic versus parasympathetic, thoracolumbar versus craniosacral outflow); the upper motor neuron (UMN) versus lower motor neuron (LMN) distinction as it applied to neurogenic bladder (SCI-06); autonomic dysreflexia (SCI-05) since bowel distension is the second most common trigger.
- Runtime: approximately 1 hour 32 minutes.
- Topic in one line: the enteric nervous system (ENS) as the autonomous “second brain,” the four-pathway extrinsic innervation (vagal, sacral parasympathetic, thoracolumbar sympathetic, pudendal somatic), the internal anal sphincter (IAS) and external anal sphincter (EAS) split, the UMN-versus-LMN bowel classification driven by the integrity of the sacral reflex arc, the bowel program (timing, positioning, bisacodyl suppository, digital stimulation versus manual evacuation), the gastrocolic and rectocolic reflexes, the acute GI complications (adynamic ileus, Ogilvie syndrome with the 12 cm cecal threshold and neostigmine 2 mg IV, superior mesenteric artery (SMA) syndrome with the aortomesenteric angle <22°, sigmoid volvulus), transanal irrigation, the Malone antegrade continence enema, and colostomy as the rescue option.
Sacral nerve stimulation (SNS) and emerging therapies. Sacral neuromodulation delivers low-amplitude electrical stimulation to the S3 nerve root via a percutaneous lead, modulating the afferent pelvic input that drives reflex detrusor overactivity and reflex bowel patterns. FDA-approved for refractory urge incontinence, idiopathic non-obstructive urinary retention, and fecal incontinence, SNS has growing off-label use for neurogenic bowel in incomplete SCI. Abdominal surface electrical stimulation is a non-invasive alternative under investigation. IV neostigmine (with glycopyrrolate) is an emerging investigational option for refractory obstipation: neostigmine inhibits acetylcholinesterase to stimulate colonic motility, while glycopyrrolate — a quaternary amine that does not readily cross the blood-brain barrier — blocks the unwanted peripheral muscarinic effects (bradycardia, bronchospasm) without causing central anticholinergic effects. Because it blocks peripheral muscarinic receptors throughout the body, glycopyrrolate does antagonize gastrointestinal muscarinic activity and can dampen gut motility; sugammadex reversal has been associated with faster gastrointestinal recovery than the neostigmine/glycopyrrolate combination. Use is monitored and not yet first-line.
Vignette. A 24-year-old man with a C6 American Spinal Injury Association Impairment Scale (AIS) A complete tetraplegia sustained 18 days ago in a motor vehicle collision is now on the acute rehabilitation unit. He has not had a bowel movement in 5 days. His abdomen is distended but soft, bowel sounds are present, and he is tolerating a regular diet. A bisacodyl 10 mg suppository was placed yesterday with no result. Digital stimulation was attempted but produced no response. He has lost 9 kg since admission and complains of bilious emesis after lunch.
Which type of neurogenic bowel pattern do you anticipate once spinal shock fully resolves, why did the suppository plus digital stimulation produce no result on day 18 post-injury, what is the likely diagnosis behind the bilious emesis and weight loss, and what is your stepwise plan to restart effective bowel evacuation?
Section 1: GI Neuroanatomy and the Two Sphincters
Bottom line: the gut runs on a 100-million-neuron enteric nervous system that survives complete spinal cord injury, modulated by four extrinsic pathways (vagal, sacral parasympathetic, sympathetic, pudendal); continence depends on a smooth-muscle internal anal sphincter (70-85% of resting tone) and a striated external anal sphincter (15-30%, voluntary).
The gastrointestinal tract carries more intrinsic neural control than any other organ system below the brainstem. The enteric nervous system (ENS) is an intrinsic neural network embedded in the gut wall from esophagus to anus, containing approximately 100 million neurons (more than the entire human spinal cord) and is capable of coordinating peristalsis, secretion, and absorption entirely independent of extrinsic innervation. Two principal plexuses do the work. Auerbach (myenteric) plexus sits between the longitudinal and circular smooth-muscle layers and is motor: it regulates the amplitude and frequency of peristaltic contractions that propel luminal contents in the aboral direction. Meissner (submucosal) plexus sits in the submucosa and is sensory and secretory: it detects luminal distension and chemical stimuli and modulates mucosal blood flow, fluid secretion, and absorption.
The clinical importance of the ENS for neurogenic bowel cannot be overstated. Even after a complete spinal cord injury the ENS continues to coordinate local peristalsis, which is why patients with LMN areflexic bowel still experience slow stool transit. A board question may present a patient with a complete cauda equina lesion and ask why any stool transit occurs at all when the sacral reflex arc is destroyed; the answer is autonomous ENS function.
Parasympathetic innervation divides anatomically into two pathways. The vagus nerve (cranial nerve X) provides parasympathetic supply from the esophagus to roughly the mid-transverse colon at the splenic flexure, increasing motility, relaxing sphincters, and stimulating secretion. Because the vagus arises in the brainstem and travels outside the spinal cord, vagal-mediated motility in the proximal and mid-colon is preserved at every spinal cord injury level. The pelvic nerve (S2-S4) carries sacral parasympathetic fibers to the descending colon, sigmoid colon, and rectum, increasing distal colonic motility and relaxing the IAS to permit defecation. Pelvic nerve function fails whenever a lesion destroys the S2-S4 segments, the defining feature of LMN bowel.
Sympathetic innervation to the gut arises from the thoracolumbar cord at T12-L2 and reaches the bowel through the hypogastric nerve and the superior and inferior mesenteric ganglia. Every sympathetic effect on the bowel promotes storage: motility slows, the IAS contracts, and secretion decreases. Somatic innervation of the EAS comes from the pudendal nerve (S2-S4); the pudendal nerve also carries sensory afferents from the perianal skin and anal canal, providing the conscious sensation of rectal fullness.
The two sphincters are functionally distinct and are tested as a pair on every neurogenic bowel question. The internal anal sphincter (IAS) is smooth muscle under involuntary autonomic control: sympathetic input contracts it and parasympathetic input relaxes it. The IAS provides 70-85% of resting anal pressure and is the workhorse of continence at rest. It relaxes reflexively in response to rectal distension through the rectoanal inhibitory reflex. The external anal sphincter (EAS) is striated skeletal muscle under voluntary somatic control via the pudendal nerve and provides 15-30% of resting pressure; it is the on-demand voluntary squeeze that allows conscious deferral of defecation when the urge arrives at a socially inconvenient moment.
In UMN bowel, the EAS becomes spastic and the patient cannot voluntarily relax it, creating a functional outlet obstruction. In LMN bowel, the EAS becomes flaccid and denervated, the voluntary guard is lost, and passive incontinence is the dominant problem. Understanding which sphincter is the “workhorse” (IAS) and which is the “guard” (EAS) is the foundation for everything that follows.

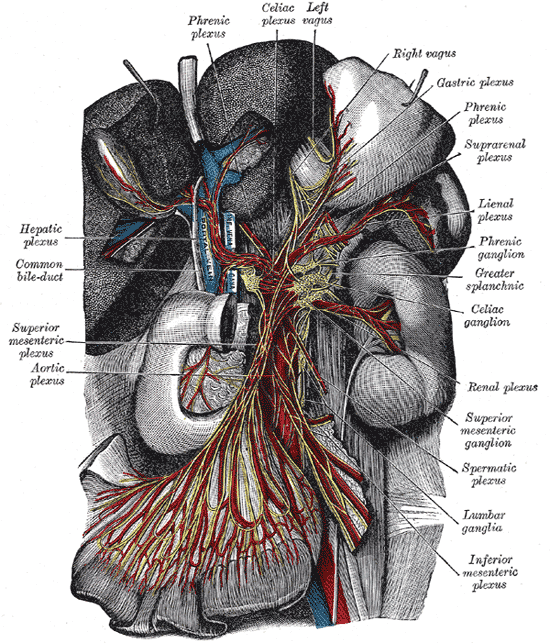
Source: Henry Gray, Anatomy of the Human Body (1918), Plate 848 via Wikimedia Commons (public domain).
High Yield — GI innervation and the two sphincters

- Enteric nervous system = ~100 million neurons, two plexuses (Auerbach = motor, Meissner = sensory/secretory); autonomous function preserved even after complete SCI.
- Vagus (CN X) supplies esophagus to mid-transverse colon and is never affected by SCI because it bypasses the spinal cord entirely.
- Pelvic nerve (S2-S4) supplies descending colon, sigmoid, rectum; lost in cauda equina/conus injury.
- Sympathetic (T12-L2) promotes storage: slows motility, contracts IAS, decreases secretion.
- Pudendal nerve (S2-S4) controls EAS plus perianal sensation.
- IAS provides 70-85% of resting anal pressure (smooth, involuntary); EAS provides 15-30% (striated, voluntary). This split is tested directly.