Respiratory Management
SCI · EP 08 · PULMONARY
Before You Listen
- Prerequisites: segmental innervation of the cervical and thoracic cord (SCI-01); the upper motor neuron (UMN) versus lower motor neuron (LMN) distinction; basic pulmonary physiology (forced vital capacity (FVC), tidal volume, the inspiratory and expiratory phases of cough); the autonomic nervous system framework from SCI-05; basic ventilator vocabulary (tidal volume, fraction of inspired oxygen, positive end-expiratory pressure).
- Runtime: approximately 56 minutes 28 seconds.
- Topic in one line: the segmental respiratory muscle map (diaphragm at C3-C5, intercostals at T1-T11, abdominals at T6-T12, accessory muscles at cranial nerve XI and C2-C4), why pneumonia is the leading cause of death across every era of SCI care, the paradoxical breathing pattern, the counterintuitive rise in FVC as intercostal spasticity emerges, the supine-versus-upright positional paradox, the abdominal binder rule (helps when upright, harms when supine), peak cough flow (PCF) thresholds and the manually assisted (“quad”) cough, mechanical insufflation-exsufflation (MI-E) pressures, progressive ventilator-free breathing (PVFB) as the SCI weaning standard, phrenic nerve pacing candidacy (C1-C2 yes, C3-C5 LMN damage no), glossopharyngeal (frog) breathing, the Passy-Muir speaking valve, and the 60% prevalence of obstructive sleep apnea in tetraplegia.
Vignette. A 32-year-old man sustained a C4 American Spinal Injury Association Impairment Scale (AIS) A complete spinal cord injury (SCI) in a diving accident 3 days ago. He is breathing spontaneously through a tracheostomy with mild support, but his forced vital capacity (FVC) is 42% of predicted, his respiratory rate is 24, and you can see his chest wall collapsing inward during inspiration while his abdomen protrudes. Suctioning produces moderate thick yellow secretions, and his peak cough flow (PCF) is 95 L/min. Oxygen saturation is 93% on a fraction of inspired oxygen of 0.4. He has not required full mechanical ventilator support but is visibly tiring. Phrenic nerve conduction studies were ordered.
Name the breathing pattern and explain why it occurs. Will his FVC improve or worsen over the coming weeks if no neurologic recovery occurs, and why? Which airway-clearance strategies should you initiate immediately, and which adjunct (binder, position) should be added in the wheelchair? Is he a candidate for phrenic nerve pacing, and what single anatomic finding determines candidacy?
Section 1: Respiratory Muscle Innervation by Spinal Level
Bottom line: every respiratory consequence of SCI flows from one map (diaphragm C3-C5 phrenic = 65-75% of tidal volume, intercostals T1-T11, abdominals T6-T12 = forced expiration and cough, accessory muscles via cranial nerve XI plus C2-C4 spared in cervical SCI); know the level, predict the FVC and the cough.
Respiratory complications are the leading cause of morbidity and mortality in both the acute and chronic phases of spinal cord injury. Pneumonia is the number one cause of death in persons with SCI across all time periods, whether measured in the first year after injury or decades later. Respiratory failure accounts for approximately 42% of acute-phase deaths. The severity of respiratory impairment maps directly onto the level and completeness of injury, and that map is built from the segmental innervation of each respiratory muscle group. Memorize the wiring and you can predict the FVC, the cough, and the ventilator picture before you walk into the room.
The diaphragm is the principal muscle of inspiration, generating approximately 65-75% of tidal volume during quiet breathing. It is innervated by the phrenic nerve, which arises from the C3, C4, and C5 nerve roots. The mnemonic that every medical student learns is “C3, C4, C5 keeps the diaphragm alive.” The phrenic nerve is a pure motor nerve to the diaphragm with sensory branches to the central diaphragm, pericardium, and peritoneal surfaces.
The clinical implications follow directly. Injuries at C1-C2 sit above all phrenic motor neurons, producing complete diaphragmatic paralysis and ventilator dependence. Injuries at C3-C4 produce partial diaphragmatic weakness because some but not all phrenic motor neurons may be damaged; many of these patients require at least temporary ventilatory support. Injuries at C5 and below spare the diaphragm because the phrenic motor neurons have already sent their axons into the phrenic nerve, though loss of accessory muscles, intercostals, and abdominals still impairs respiratory mechanics.
The intercostal muscles are innervated segmentally by the intercostal nerves at T1-T11. The external intercostals are inspiratory; they elevate the ribs during inspiration to expand the thoracic cavity. The internal intercostals (interosseous portion) depress the ribs during forced expiration; the parasternal portion is paradoxically inspiratory. In cervical SCI, complete intercostal paralysis means the chest wall cannot stabilize during inspiration, which is the mechanism of paradoxical breathing.
The abdominal muscles are the primary muscles of forced expiration and cough, innervated at T6-T12 with some contribution from T5. Rectus abdominis (T7-T12), external oblique (T7-T12), internal oblique and transversus abdominis (T7-L1) generate the high intrathoracic pressures required for an effective cough. Their paralysis in cervical and high thoracic SCI is the primary reason for impaired secretion clearance and the resulting susceptibility to atelectasis and pneumonia.
The accessory muscles of respiration are spared in cervical SCI because their innervation comes from cranial nerves and the highest cervical segments. The sternocleidomastoid is innervated primarily by the spinal accessory nerve (cranial nerve XI) with contributions from C2-C3. The trapezius is innervated by cranial nerve XI plus C3-C4 and stabilizes the scapula. The scalenes (C3-C8) elevate ribs 1 and 2. In high cervical SCI at C1-C4, the sternocleidomastoid and trapezius become the principal available respiratory muscles, but accessory muscles alone are insufficient to sustain ventilation in most complete C1-C2 injuries.
The respiratory consequences by level cluster into bands. C1-C2 leaves only the sternocleidomastoid and trapezius available; FVC drops to 5-10% of predicted and patients are ventilator-dependent. C3-C4 produces partial diaphragm function with FVC at 15-30%; most patients require acute ventilatory support but some may eventually wean. C5-C8 preserves the diaphragm but loses intercostal and abdominal function; cough is severely impaired and FVC sits at roughly 30-50%. T1-T5 preserves the diaphragm and partial intercostal function with moderately impaired cough and FVC at 50-75%. T6-T12 preserves diaphragm, intercostals, and partial abdominal muscles with mildly impaired cough and FVC at 75-90%. L1 and below leaves all respiratory muscles intact with no significant respiratory impairment from the SCI itself.

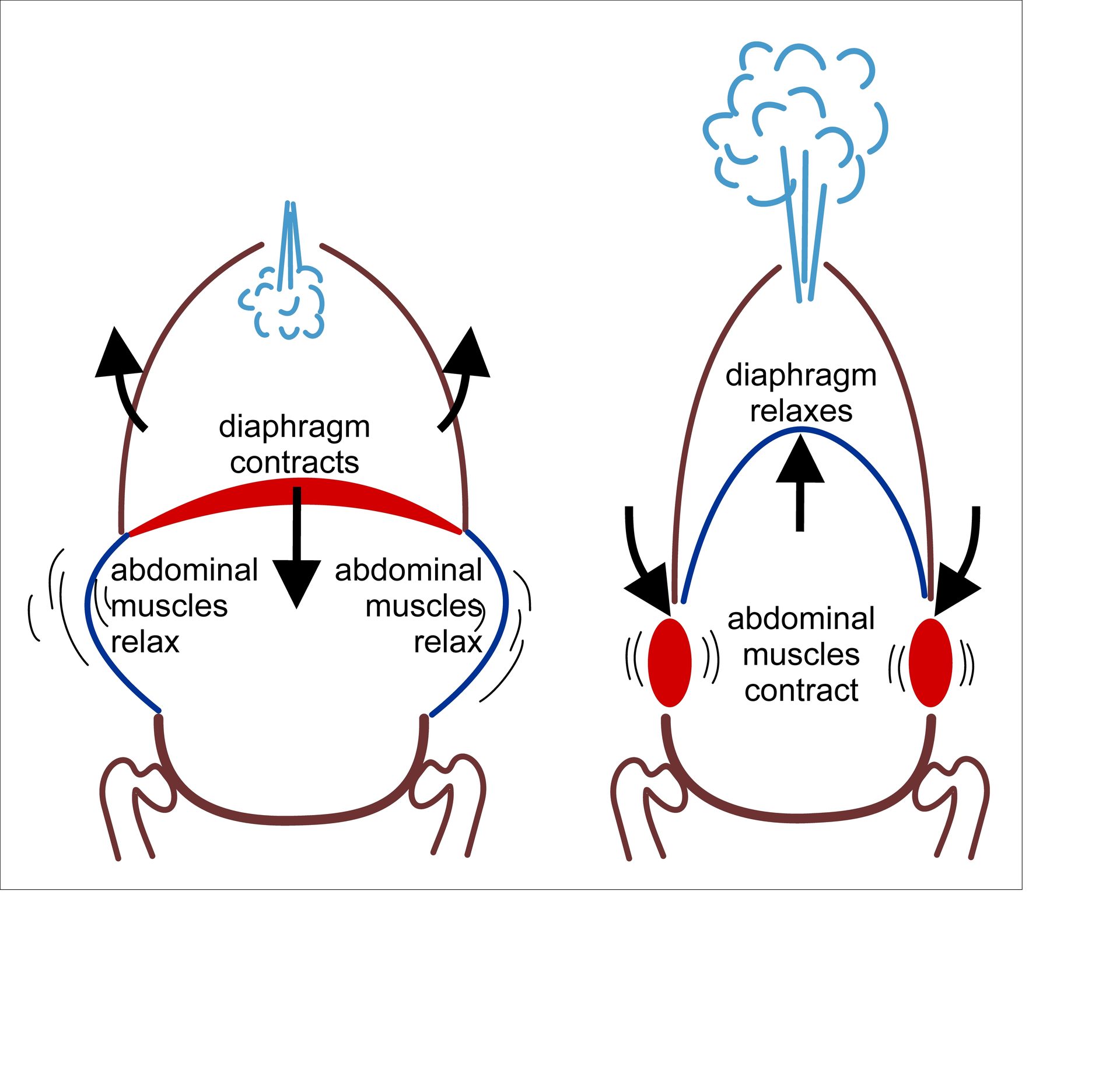
Source: Wikimedia Commons, “Muscles involved in forceful breathing in and out” by Theresa Knott (CC BY-SA 4.0).
High Yield — Innervation map and FVC by level
- Phrenic = C3, C4, C5, generates 65-75% of tidal volume; “C3, C4, C5 keeps the diaphragm alive.”
- Intercostals T1-T11, external = inspiratory, internal interosseous = expiratory; loss = paradoxical breathing.
- Abdominals T6-T12, the engine of forced expiration and cough; loss = the cardinal driver of atelectasis and pneumonia.
- Accessory muscles (SCM, trapezius) receive cranial nerve XI input and are preserved in cervical SCI; this is why C4-C5 patients often look like they are “using everything in their neck” to breathe.
- Predicted FVC by level: C1-C2 ≈ 5-10%, C3-C4 ≈ 15-30%, C5-C8 ≈ 30-50%, T1-T5 ≈ 50-75%, T6-T12 ≈ 75-90%.