Pressure Injuries in Spinal Cord Injury
SCI · EP 12 · PRESSURE
Before You Listen
This episode covers the National Pressure Injury Advisory Panel (NPIAP) staging system, the rule against reverse staging, the pressure-shear-friction physics that kills muscle faster than skin, the geographic risk map by body position with the ischial tuberosities as the most common SCI site, the Braden Scale and its ceiling-effect limitation in complete SCI, the prevention numbers (15–30 minute pressure relief, 45-degree wheelchair tilt for 1–2 minutes, 30-degree lateral bed positioning every 2 hours, 1.25–1.5 g/kg/day protein), moist wound healing principles, negative pressure wound therapy parameters, surgical flap selection by site with the postoperative sitting protocol, and the four life-threatening complications (osteomyelitis, sepsis, Marjolin ulcer, secondary amyloidosis).
What you should already know coming in:
- The autonomic dysreflexia (AD) trigger algorithm from Episode 5: pressure injury and acute abdomen are deep-search triggers after bladder and bowel are cleared.
- Neurogenic bowel and bladder programs from Episodes 6 and 7, because moisture management directly reduces pressure injury risk.
- The American Spinal Injury Association (ASIA) Impairment Scale (AIS) grades and the concept that complete sensory loss eliminates protective discomfort signaling.
Runtime: approximately 1 hour 30 minutes.
Vignette. A 42-year-old woman with a 9-year-old T4 American Spinal Injury Association (ASIA) Impairment Scale (AIS) A complete paraplegia is admitted from a community wheelchair clinic with a new wound over her right ischial tuberosity. On examination, the wound is 4 cm by 3 cm with a crater depth of 2.5 cm. Subcutaneous adipose tissue is clearly visible in the wound bed, with rolled epibole edges and approximately 30% slough; no bone, tendon, or muscle is exposed or palpable on probe-to-bone testing. Surrounding skin is warm but not fluctuant, and there is no purulent drainage. Her Braden Scale score is 9 (sensory perception 1, mobility 1, activity 1, nutrition 2, moisture 2, friction and shear 2). Serum albumin is 2.9 grams per deciliter (g/dL); prealbumin is 12 milligrams per deciliter (mg/dL). She smokes half a pack per day and uses a standard foam wheelchair cushion.
Stage this pressure injury, explain why a Braden score of 9 is misleading in this patient and which subscales drive your interventions, list the prevention numbers you would change today (cushion, sitting tilt, repositioning, nutrition, smoking), explain whether and when you would offer surgical flap closure, and state the documentation rule you must follow if this wound heals.
(Answer at the end of this chapter)
Section 1: NPIAP Staging — Four Stages, Two Categories, and the No-Reverse-Staging Rule
Bottom line: the NPIAP system has 4 numerical stages and 2 additional categories (unstageable, deep tissue pressure injury), the boundary between stage 2 and stage 3 is the appearance of slough or eschar, the boundary between stage 3 and stage 4 is exposed bone/tendon/muscle, and a healed stage 4 is documented forever as “healing stage 4,” never restaged downward.
Pressure injuries are the most common, costly, and preventable complication of spinal cord injury (SCI). The lifetime incidence ranges from 25% to 85%. At any given time, approximately 20–30% of community-dwelling individuals with SCI carry at least one pressure injury. Pressure injuries are the most common reason for rehospitalization after initial SCI rehabilitation discharge, accounting for ~30% of readmissions. Treating a single stage 4 injury costs $20,000 to over $150,000. Mortality in SCI patients with pressure injuries is 2 to 5 times higher than in those without; sepsis from infected pressure injuries is a leading cause of death in chronic SCI.
The National Pressure Injury Advisory Panel (NPIAP) staging system was renamed from the National Pressure Ulcer Advisory Panel (NPUAP) in 2016, when the term “pressure ulcer” was replaced with “pressure injury” and the stage definitions were refined. The system has 4 numerical stages plus 2 additional categories (unstageable and deep tissue pressure injury, DTPI). Stage 1 is non-blanchable erythema of intact skin. The skin is intact with no break in the epidermis. Non-blanchable erythema persists after pressure release. The board-favorite distinction: pressing a finger on blanchable erythema turns the skin white and it returns to red on release (reactive hyperemia, normal); non-blanchable erythema stays red under finger pressure because red blood cells have already extravasated into the interstitium (tissue damage has already occurred). In darkly pigmented skin, visible erythema may not be apparent and the clinician must rely on temperature, firmness, and pain changes versus surrounding tissue.
Stage 2 is partial-thickness skin loss with exposed dermis. The wound bed is viable, pink or red, and moist. An intact or ruptured serum-filled blister qualifies. Granulation tissue, slough, and eschar are NOT present in stage 2. If they are, the injury cannot be staged as 2. This stage is also not used for moisture-associated skin damage, medical adhesive-related skin injury, or skin tears unrelated to pressure and shear.
Stage 3 is full-thickness skin loss with adipose tissue visible in the wound bed. Granulation tissue and rolled wound edges (epibole) are often present. Bone, tendon, and muscle are not exposed; if they are, the injury is stage 4. Undermining and tunneling may occur. Depth varies by anatomic location: buttocks can develop deep stage 3 injuries, while the occiput or malleolus may be quite shallow.
Stage 4 is full-thickness skin and tissue loss with exposed or directly palpable bone, tendon, muscle, ligament, cartilage, or joint capsule. Slough or eschar may be present. Undermining and tunneling are often extensive. The injury can extend into supporting structures, making osteomyelitis possible.
Unstageable injuries are full-thickness with the wound base obscured by slough or eschar (slough may be yellow, tan, gray, green, or brown; eschar may be tan, brown, or black). The true depth cannot be determined until enough is removed; the wound is then revealed as either stage 3 or stage 4. Deep tissue pressure injury (DTPI) presents as intact or non-intact skin with localized persistent non-blanchable deep red, maroon, or purple discoloration, or epidermal separation revealing a dark wound bed or blood-filled blister. It results from intense or prolonged pressure and shear at the bone-muscle interface; pain and temperature change often precede skin color changes. The 2016 revision dropped the word “suspected” from the DTPI designation. A DTPI may evolve rapidly to full-thickness injury despite optimal treatment.
The single most-tested documentation principle is the no-reverse-staging rule. A stage 4 pressure injury that is healing is documented forever as a healing stage 4, not restaged down to 3, 2, then 1. Deep injuries heal by secondary intention: granulation tissue forms, the wound contracts, and re-epithelialization closes the surface. The lost muscle, subcutaneous fat, and dermis are replaced by scar tissue, not by regeneration of the original tissue layers. Scar regains a maximum of about 80% of the tensile strength of native skin, lacks normal elasticity, has reduced vascularity, and lacks the sweat glands and subcutaneous architecture needed to regulate local microclimate. Restaging downward would falsely communicate that the tissue has the resilient architecture of a superficial wound, leading to under-protection. Progress is documented by serial wound dimensions (length, width, depth in centimeters), the percentage of wound bed covered by granulation versus slough/eschar, reduction in undermining and tunneling, and advancement of wound edges.

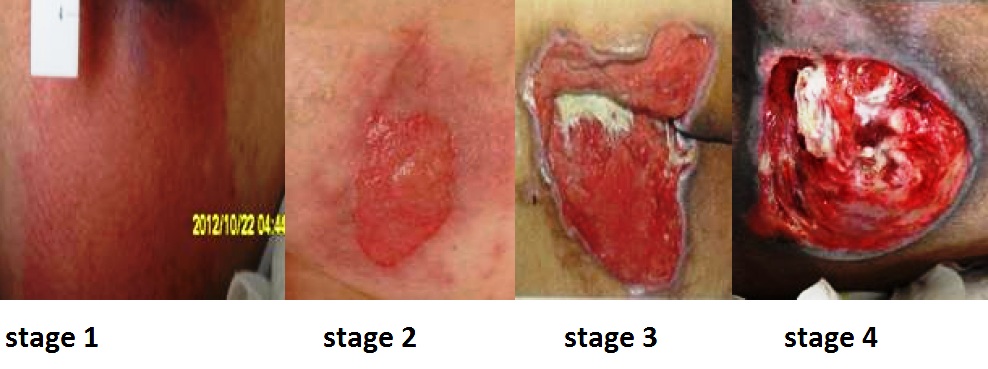
Source: Babagolzadeh, “Stages of wound in pressure ulcer”, via Wikimedia Commons, CC BY-SA 3.0. https://commons.wikimedia.org/wiki/File:Wound_stage.jpg
High Yield — NPIAP staging boundaries
- Stage 1 → Stage 2 boundary: the epidermis breaks. Blanchable erythema is NOT a pressure injury.
- Stage 2 → Stage 3 boundary: appearance of slough/eschar OR adipose tissue in wound bed.
- Stage 3 → Stage 4 boundary: bone, tendon, muscle, ligament, cartilage, or joint capsule exposed or palpable.
- Unstageable: can’t see the bottom because slough/eschar covers it.
- DTPI: intact-skin discoloration; injury at the bone-muscle interface; pain and temperature change precede color change.
- NO reverse staging. Healing stage 4 is forever a healing stage 4.
- Lifetime incidence after SCI: 25–85%; ~30% of SCI rehospitalizations.