Sexuality, Fertility, and Reproductive Health
SCI · EP 13 · NEUROUROLOGY
Before You Listen
- Prerequisites: sacral reflex arc anatomy, sympathetic and parasympathetic outflow tracts, and Rexed laminae from SCI-01; autonomic dysreflexia (AD) physiology, the T6 watershed, and first-line nifedipine from SCI-05; neurogenic bladder and bowel management from SCI-08 and SCI-09.
- Runtime: 1 hour 4 minutes.
- Topic in one line: the Point and Shoot mnemonic; parasympathetic erection at S2 through S4 via the pelvic nerve; sympathetic ejaculation at T11 through L2 via the hypogastric nerve; reflexogenic versus psychogenic erections by injury pattern; phosphodiesterase type 5 (PDE5) inhibitor pharmacology with the absolute nitrate contraindication; the male infertility duo of ejaculatory dysfunction plus poor semen quality; leukocytospermia as the single worst predictor; the sperm retrieval ladder (penile vibratory stimulation [PVS], electroejaculation [EEJ], surgical retrieval); female fertility preservation; post-injury amenorrhea; contraception choices that respect deep vein thrombosis (DVT) and autonomic dysreflexia (AD) risk; the 85 to 90 percent AD-during-labor rate above T6; epidural to T10 as the treatment of choice; and the AD versus preeclampsia bedside differential.
Vignette. A 28-year-old man with C7 motor-complete tetraplegia (American Spinal Injury Association Impairment Scale [AIS] A), 1 year post-injury, presents with his partner to discuss starting a family. He gets firm erections from direct genital touch but cannot get an erection from erotic thoughts alone, and he has never ejaculated during sexual activity. He uses sildenafil 50 mg occasionally to improve rigidity. The couple has had unprotected intercourse for 6 months without conception. His semen analysis: sperm count 92 million/mL, motility 12 percent, white blood cells 3.4 million/mL.
Which type of erection is preserved and why? What is the expected ejaculation rate at his injury level? What is the first-line sperm retrieval method, and what is the AD precaution? Which AD treatment is absolutely contraindicated for him, and why? What does his semen analysis tell you about his fertility prognosis?
Section 1: Neuroanatomy of Sexual Function and the Point and Shoot Map
Bottom line: parasympathetic at S2 through S4 via the pelvic nerve points (erection); sympathetic at T11 through L2 via the hypogastric nerve shoots (ejaculation); the somatic pudendal nerve at S2 through S4 carries genital sensation and drives the expulsion phase. Memorize the four numbers and the four nerves cold. Nearly every sexual-function question on the boards reduces to this map.
Before you can predict what survives a given spinal cord injury (SCI), you need a clean wiring diagram. Sexual response in both sexes is controlled by two autonomic centers and one somatic nerve.
The parasympathetic erection center sits in the intermediolateral cell column at S2 through S4. Preganglionic fibers travel through the pelvic nerve (the nervi erigentes) to the cavernous nerves of the corpora cavernosa. Firing releases nitric oxide from non-adrenergic non-cholinergic terminals and endothelial cells. Nitric oxide activates guanylate cyclase, which raises intracellular cyclic guanosine monophosphate (cGMP). cGMP relaxes trabecular smooth muscle; arterial inflow surges, the sinusoids engorge, and the expanding tissue compresses the subtunical venules against the inelastic tunica albuginea. That veno-occlusive mechanism produces a rigid erection. Every step matters because PDE5 inhibitor pharmacology targets the cGMP step directly.
The sympathetic ejaculation center sits at T11 through L2. Postganglionic fibers travel through the hypogastric nerve to the pelvic organs. Sympathetic activation drives the emission phase: contraction of the vas deferens and seminal vesicles propels seminal fluid into the posterior urethra, while the internal urethral sphincter contracts to close the bladder neck and prevent retrograde ejaculation. The expulsion phase then follows, driven by rhythmic contraction of the bulbospongiosus and ischiocavernosus muscles via the somatic pudendal nerve at S2 through S4.
The pudendal nerve carries three jobs: sensory afferents from the genitalia (trigger for the sacral reflex arc), motor efferents to pelvic floor expulsion muscles, and the bulbocavernosus reflex you test at the bedside. Both erection and ejaculation depend on S2 through S4 in part, but the autonomic drivers are cleanly separated. Point and Shoot.

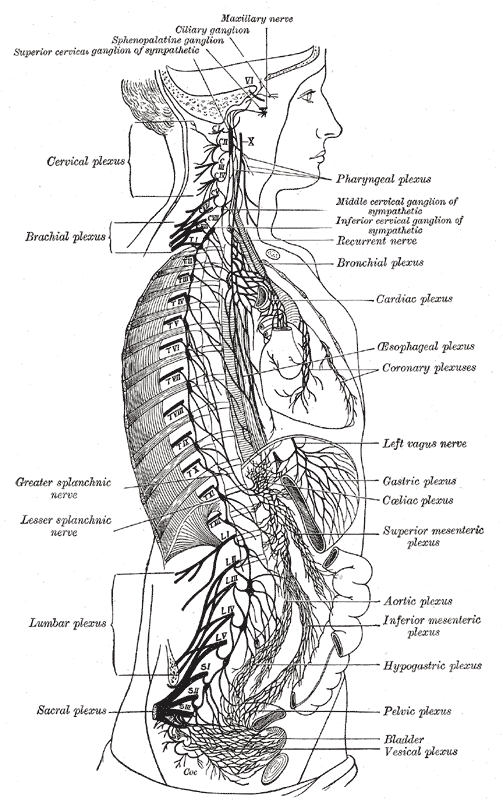
Source: Henry Gray, Anatomy of the Human Body (1918), Plate 838 via Wikimedia Commons (public domain).
High Yield: Point and Shoot
- Parasympathetic = Point = Erection: S2 through S4 via the pelvic nerve.
- Sympathetic = Shoot = Ejaculation: T11 through L2 via the hypogastric nerve.
- Pudendal nerve (S2 through S4, somatic): genital sensation and the expulsion phase.
- Erection cascade: NO -> guanylate cyclase -> cGMP -> smooth muscle relaxation -> veno-occlusion.
- Ejaculation: emission (sympathetic, bladder neck closes) + expulsion (pudendal-driven).
It’s a closed loop. The defining characteristic of a reflexogenic erection is that it requires absolutely zero input from the brain. The patient does not need to be experiencing mental arousal. It is a spinal reflex, plain and simple.
— SCI-13 podcast, ~14:04