Spasticity and Motor Recovery
TBI · EP 10 · NEUROREHABILITATION
Before You Listen
- Prerequisites: the upper motor neuron (UMN) syndrome (positive vs negative features); the GABA-A vs GABA-B receptor distinction; the gamma motor neuron and muscle spindle stretch reflex; the basics of botulinum toxin chemodenervation; and Wolff’s law in bone remodeling.
- Runtime: 1 hour 14 minutes.
- Topic in one line: spasticity defined as a velocity-dependent increase in tonic stretch reflexes (Lance, 1980), the velocity-dependent vs velocity-independent (rigidity) vs structural (contracture) distinction, the Modified Ashworth Scale (MAS) with the diagnostic 1+ grade, the Modified Tardieu Scale with the R2 minus R1 dynamic-vs-structural arithmetic, the Penn Spasm Frequency Scale, the noxious stimulus search, the paradox of tone (when spasticity is functionally beneficial), oral medications (baclofen, tizanidine, dantrolene, gabapentin) with their receptor targets and signature adverse effects, botulinum toxin and the SNARE-cleavage mechanism (SNAP-25 vs synaptobrevin), the inject-and-cast technique, intrathecal baclofen (ITB) therapy with the lethal withdrawal triad, phenol/alcohol neurolysis, the equinovarus deformity and SPLATT procedure, the 12 to 18 month neurologic plateau before surgery, and motor recovery via diaschisis resolution and cortical remapping.
Vignette. A 24-year-old woman, 8 weeks after a severe traumatic brain injury (TBI) from a high-speed motor vehicle collision, has been transferred to acute inpatient rehabilitation. She is at Rancho Los Amigos Level 5 and follows simple commands. Her left ankle is held in plantarflexion and inversion that interferes with shoe wear and prevents heel strike during gait training. On Modified Ashworth Scale (MAS) the left gastrocnemius is grade 3. On the Modified Tardieu Scale the slow-velocity passive range of motion (R2) reaches 5° of dorsiflexion, while the fast-velocity catch (R1) occurs at 30° of plantarflexion. There is no fever; urine is clear; the bowels moved this morning; the ankle-foot orthosis is well-fitted. Her cognitive team has emphasized that she must remain alert for the structured neuropsychological program.
Name the deformity, interpret the R2 minus R1 difference, name the most likely effective focal intervention, name the synergistic mechanical add-on that should follow it within a week, and name the surgical procedure (with its acronym) that becomes an option only after the 12 to 18 month neurologic plateau if dynamic varus persists.
Section 1: Definition, Pathophysiology, and the Three-Way Tone Distinction
Bottom line: spasticity is a velocity-dependent increase in tonic stretch reflexes (Lance, 1980); it is one positive feature of the UMN syndrome; rigidity is velocity-independent and contracture is fixed structural shortening, and that three-way distinction drives every spasticity treatment decision.
Spasticity affects approximately 70% of patients with severe TBI, and untreated or undertreated tone progresses to contracture in up to 85% of severe cases. Onset is usually within weeks of injury and can appear as early as 1 week post-injury. The classic definition, per Lance (1980), is a velocity-dependent increase in tonic stretch reflexes from hyperexcitability of the stretch reflex. Velocity dependence is the cornerstone of clinical assessment and the property that separates spasticity from every other form of increased tone.
Spasticity is a positive feature of the upper motor neuron (UMN) syndrome. UMN positive features include spasticity, clonus, hyperreflexia, the Babinski sign, and spastic co-contraction. UMN negative features include weakness or paresis, loss of dexterity, and fatigability. The negative features are often more disabling, but spasticity receives disproportionate clinical attention because it is modifiable (drugs, toxins, neurolysis, surgery), while no medication restores lost dexterity.
The three-way diagnostic distinction is heavily tested. Spasticity is velocity-dependent (faster stretch = more resistance). Rigidity is velocity-independent (constant resistance at any speed; lead-pipe or cogwheel in parkinsonism). Contracture is fixed structural shortening that does not change with velocity. This distinction drives the entire treatment algorithm.
The pathophysiology after TBI involves disruption of descending inhibitory pathways from cortex, basal ganglia, and brainstem to spinal motor neurons. When the corticospinal and corticoreticular tracts are damaged, unopposed reticulospinal and vestibulospinal facilitation amplifies muscle tone. Over weeks to months, spinal cord reorganization adds denervation hypersensitivity, collateral sprouting, and altered interneuron circuitry. Prolonged spasticity drives peripheral structural changes (fibrosis, sarcomere loss, collagen deposition) that produce contracture independent of the original neural hyperexcitability. The interplay between the neural, dynamic component (responsive to pharmacology and chemodenervation) and the structural, fixed component (requiring mechanical or surgical correction) is critical for treatment selection. TBI spasticity differs from SCI or stroke spasticity in that it is frequently bilateral, affects upper and lower extremities together, and is complicated by concurrent cognitive deficits and paroxysmal sympathetic hyperactivity (PSH, covered in TBI-09).

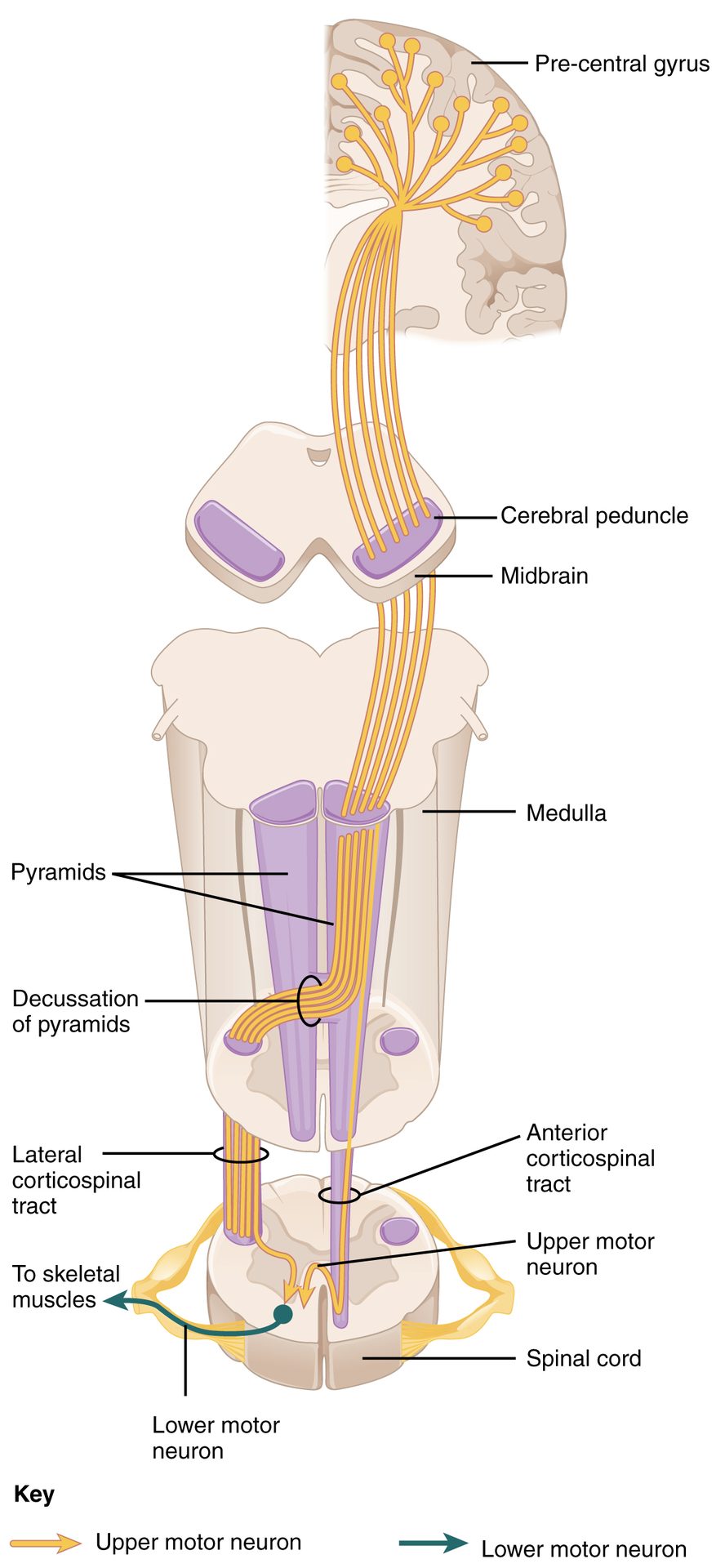
Source: OpenStax College / Anatomy & Physiology, via Wikimedia Commons (CC BY 3.0).
High Yield: Tone Definitions and the UMN Syndrome

- Spasticity (Lance, 1980): velocity-dependent increase in tonic stretch reflexes from hyperexcitability of the stretch reflex.
- UMN positive features: spasticity, clonus, hyperreflexia, Babinski, spastic co-contraction.
- UMN negative features: weakness, loss of dexterity, fatigability (often more disabling, not modifiable).
- TBI severe spasticity prevalence ~70%; contracture in untreated severe cases up to 85%.
- Three-way distinction: spasticity (velocity-dependent) vs rigidity (velocity-independent) vs contracture (fixed).
- TBI vs SCI/stroke spasticity: bilateral, upper + lower limbs, complicated by cognition and PSH.
Board Trap: Treating Without the Velocity Test

A vignette describing a stiff limb with no velocity testing is incomplete data. If a clinician orders oral baclofen for a stiff ankle without first establishing whether the resistance is velocity-dependent, they may be treating contracture (which will not respond to a GABA-B agonist) or even rigidity (a basal ganglia problem requiring dopaminergic, not anti-spastic, therapy). The first move is the Modified Ashworth Scale (MAS) for screening and the Tardieu Scale for the R2 minus R1 dynamic-vs-structural arithmetic.
If the Modified Ashworth only tests at one uniform speed of one second, how do you know what you are actually feeling in your hands? You simply don’t. The Modified Ashworth Scale is fundamentally incapable of distinguishing dynamic neural spasticity from a fixed structural contracture.
— TBI-10 podcast, ~25:46